https://www.youtube.com/watch?v=dAzOCqWUBrk
https://www.youtube.com/watch?v=dAzOCqWUBrk
https://www.youtube.com/watch?v=bgTu7MC3gVc
https://www.youtube.com/watch?v=vVX7-ptweYQ
https://www.youtube.com/watch?v=PnDC96vda2o
 The Navajo Nation was heavily impacted by the pandemic, and some of the most excess deaths occurred in Navajo County, Arizona. Here, a Navajo elder and his family pose near the town of Steamboat in neighboring Apache County, Arizona. Credit: Mark Ralston Getty Images
The Navajo Nation was heavily impacted by the pandemic, and some of the most excess deaths occurred in Navajo County, Arizona. Here, a Navajo elder and his family pose near the town of Steamboat in neighboring Apache County, Arizona. Credit: Mark Ralston Getty Images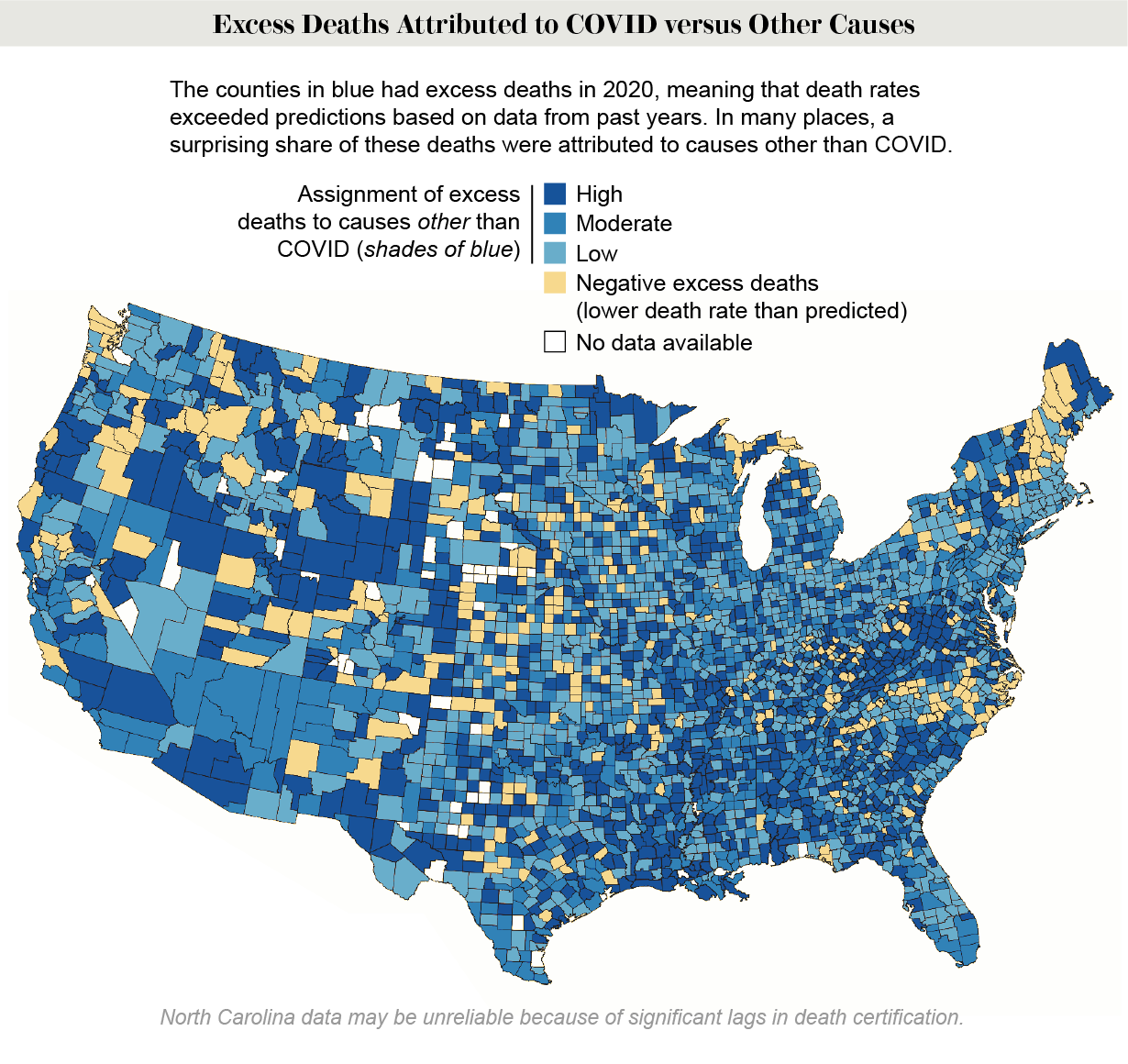 Credit: Calvin A. Ackley and Andrew C. Stokes (map); Restyled by Amanda Montañez; Source: “County-Level Estimates of Excess Mortality Associated with COVID-19 in the United States,” by Calvin A. Ackley et al. Preprint posted May 5, 2021, to www.medrxiv.org/content/10.1101/2021.04.23.21255564v2
Credit: Calvin A. Ackley and Andrew C. Stokes (map); Restyled by Amanda Montañez; Source: “County-Level Estimates of Excess Mortality Associated with COVID-19 in the United States,” by Calvin A. Ackley et al. Preprint posted May 5, 2021, to www.medrxiv.org/content/10.1101/2021.04.23.21255564v2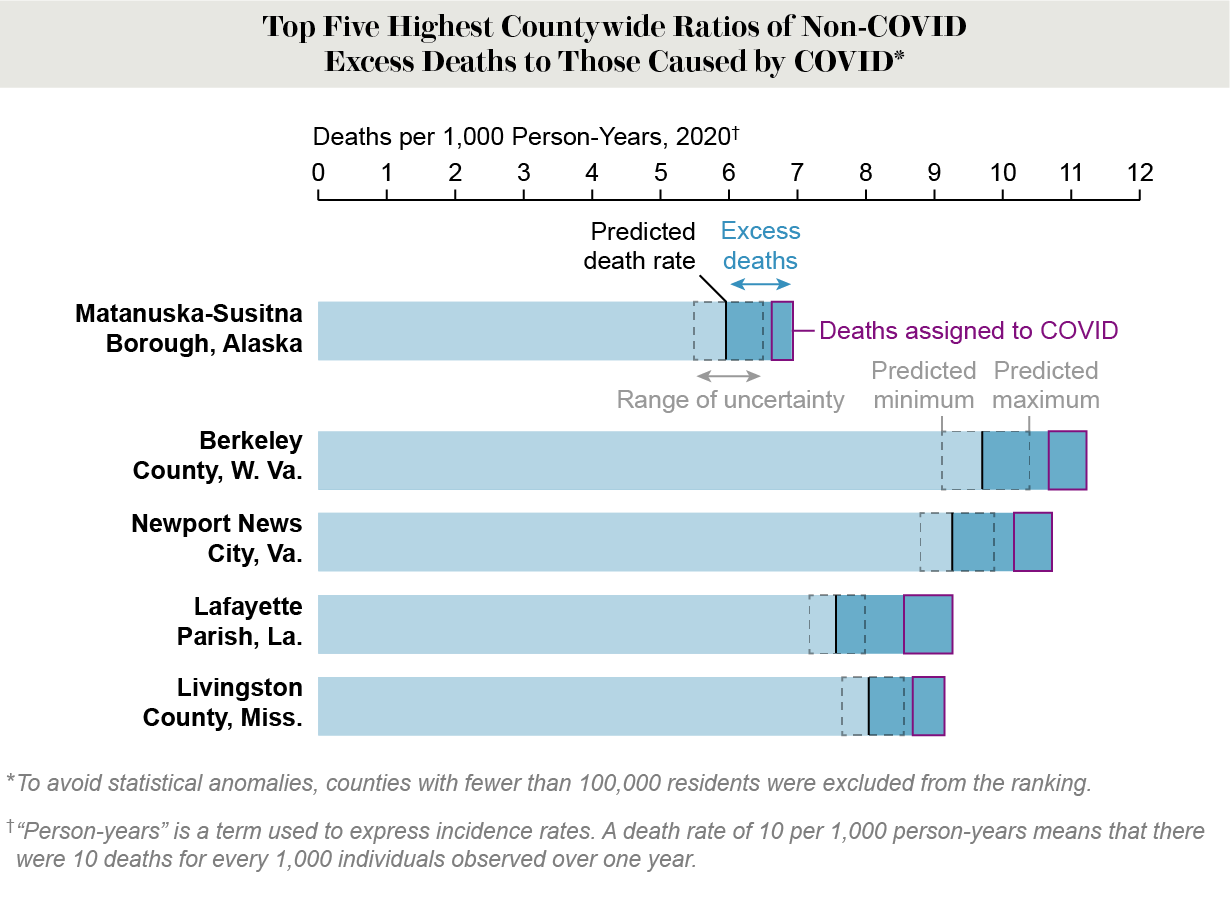 Credit: Amanda Montañez; Source: “County-Level Estimates of Excess Mortality Associated with COVID-19 in the United States,” by Calvin A. Ackley et al. Preprint posted May 5, 2021, to www.medrxiv.org/content/10.1101/2021.04.23.21255564v2
Credit: Amanda Montañez; Source: “County-Level Estimates of Excess Mortality Associated with COVID-19 in the United States,” by Calvin A. Ackley et al. Preprint posted May 5, 2021, to www.medrxiv.org/content/10.1101/2021.04.23.21255564v2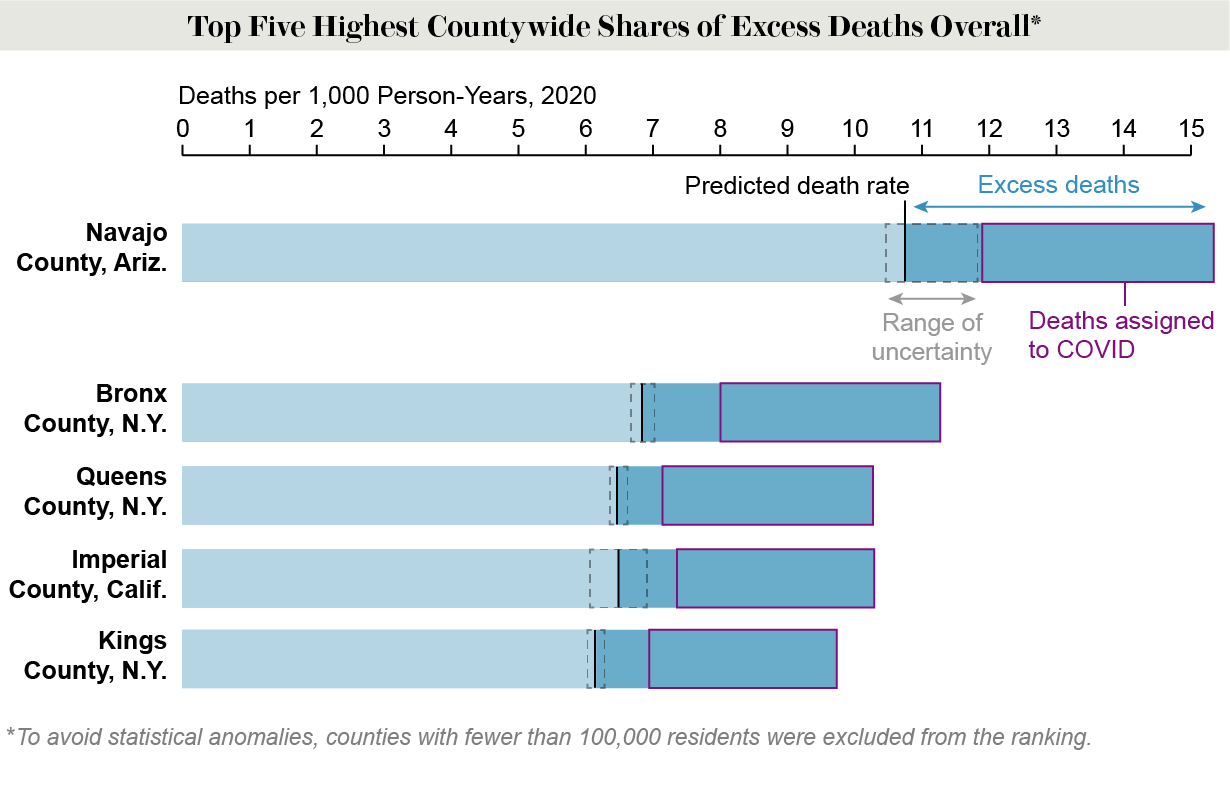 Credit: Amanda Montañez; Source: “County-Level Estimates of Excess Mortality Associated with COVID-19 in the United States,” by Calvin A. Ackley et al. Preprint posted May 5, 2021, to www.medrxiv.org/content/10.1101/2021.04.23.21255564v2
Credit: Amanda Montañez; Source: “County-Level Estimates of Excess Mortality Associated with COVID-19 in the United States,” by Calvin A. Ackley et al. Preprint posted May 5, 2021, to www.medrxiv.org/content/10.1101/2021.04.23.21255564v2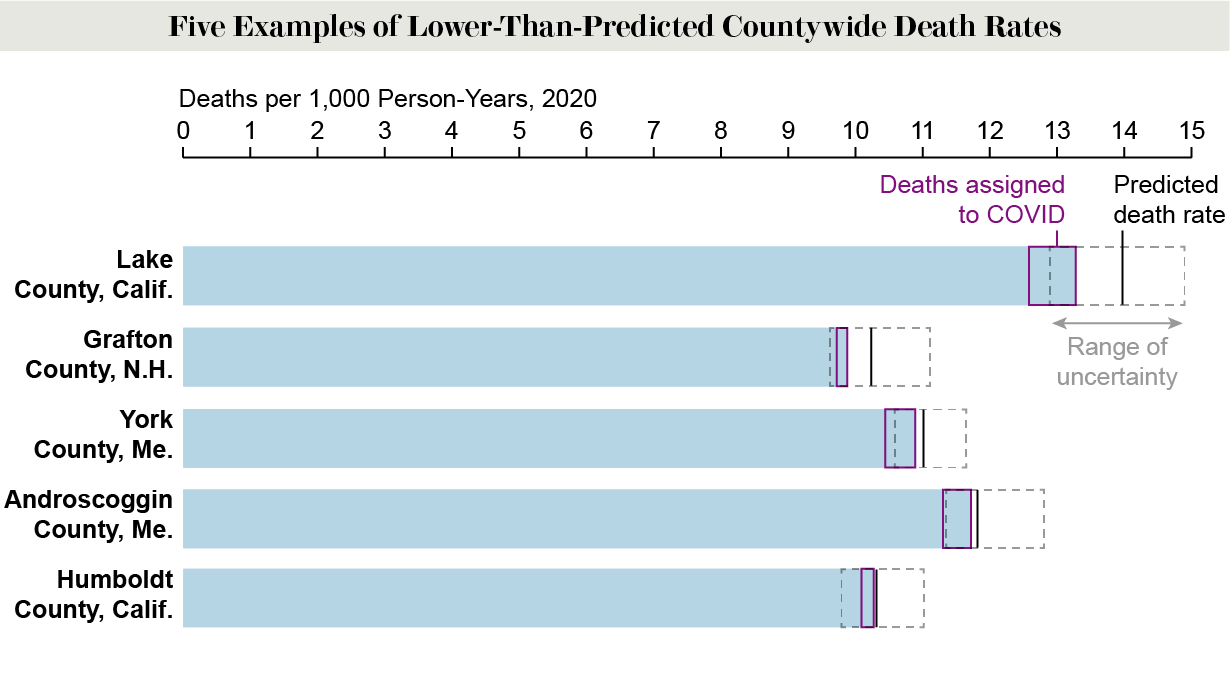 Credit: Amanda Montañez; Source: “County-Level Estimates of Excess Mortality Associated with COVID-19 in the United States,” by Calvin A. Ackley et al. Preprint posted May 5, 2021, to www.medrxiv.org/content/10.1101/2021.04.23.21255564v2
Credit: Amanda Montañez; Source: “County-Level Estimates of Excess Mortality Associated with COVID-19 in the United States,” by Calvin A. Ackley et al. Preprint posted May 5, 2021, to www.medrxiv.org/content/10.1101/2021.04.23.21255564v2
