skip to main |
skip to sidebar
https://theconversation.com/we-found-and-tested-47-old-drugs-that-might-treat-the-coronavirus-results-show-promising-leads-and-a-whole-new-way-to-fight-covid-19-136789
The more researchers know about how the coronavirus attaches, invades and hijacks human cells, the more effective the search for drugs to fight it. That was the idea my colleagues and I hoped to be true when we began building a map of the coronavirus two months ago. The map shows all of the coronavirus proteins and all of the proteins found in the human body that those viral proteins could interact with.
In theory, any intersection on the map between viral and human proteins is a place where drugs could fight the coronavirus. But instead of trying to develop new drugs to work on these points of interaction, we turned to the more than 2,000 unique drugs already approved by the FDA for human use. We believed that somewhere on this long list would be a few drugs or compounds that interact with the very same human proteins as the coronavirus.
We were right.
Our multidisciplinary team of researchers at the University of California, San Francisco, called the QCRG, identified 69 existing drugs and compounds with potential to treat COVID-19. A month ago, we began shipping boxes of these drugs off to Institut Pasteur in Paris and Mount Sinai in New York to see if they do in fact fight the coronavirus.
In the last four weeks, we have tested 47 of these drugs and compounds in the lab against live coronavirus. I’m happy to report we’ve identified some strong treatment leads and identified two separate mechanisms for how these drugs affect SARS-CoV-2 infection. Our findings were published on April 30 in the journal Nature.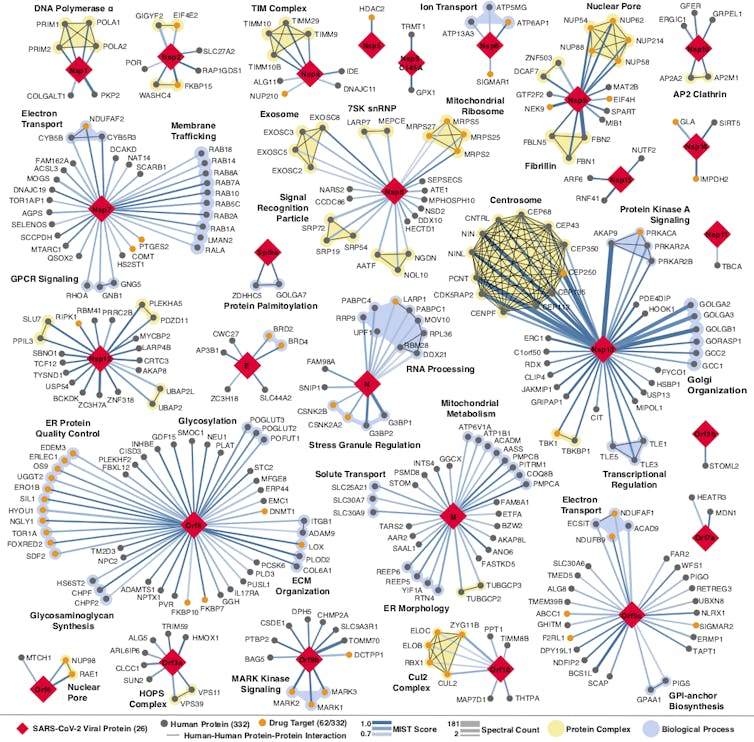 Every place that a coronavirus protein interacts with a human protein is a potential druggable site. QBI Coronavirus Research Group, CC BY-ND
Every place that a coronavirus protein interacts with a human protein is a potential druggable site. QBI Coronavirus Research Group, CC BY-ND
The testing process
The map we developed and the FDA drug catalog we screened it against showed that there were potential interactions between the virus, human cells and existing drugs or compounds. But we didn’t know whether the drugs we identified would make a person more resistant to the virus, more susceptible or do anything at all.
To find those answers we needed three things: the drugs, live virus and cells in which to test them. It would be optimal to test the drugs in infected human cells. However, scientists don’t yet know which human cells work best for studying the coronavirus in the laboratory. Instead we used African green monkey cells, which are frequently used in place of human cells to test antiviral drugs. They can be readily infected with the coronavirus and respond to drugs very closely to the way human cells do.
After infecting these monkey cells with live virus, our partners in Paris and New York added the drugs we identified to half and kept the other half as controls. They then measured the amount of virus in the samples and the number of cells that were alive. If the samples with drugs had a lower virus count and more cells alive compared to the control, that would suggest the drugs disrupt viral replication. The teams were also looking to see how toxic the drugs were to the cells. With dozens of drugs each needing full testing, to get results in four weeks required round-the-clock effort. Quantitative Biosciences Institute, CC BY-ND
With dozens of drugs each needing full testing, to get results in four weeks required round-the-clock effort. Quantitative Biosciences Institute, CC BY-ND
After sorting through the results of hundreds of experiments using 47 of the predicted drugs, it seems our interaction predictions were correct. Some of the drugs do in fact work to fight the coronavirus, while others make cells more susceptible to infection.
It is incredibly important to remember that these are preliminary findings and have not been tested in people. No one should go out and buy these drugs.
But the results are interesting for two reasons. Not only did we find individual drugs that look promising to fight the coronavirus or may make people more susceptible to it; we know, at a cellular level, why this is happening.
We identified two groups of drugs that affect the virus and they do it two different ways, one of which has never been described.
Disrupting translation
At a basic level, viruses spread by entering a cell, hijacking some of the cell’s machinery and using it to make more copies of the virus. These new viruses then go on to infect other cells. One step of this process involves the cell making new viral proteins out of viral RNA. This is called translation.
When going through the map, we noticed that several viral proteins interacted with human proteins involved in translation and a number of drugs interacted with these proteins. After testing them, we found two compounds that disrupt the translation of the virus.
The two compounds are called ternatin-4 and zotatifin. Both of these are currently used to treat multiple myeloma and seem to fight COVID-19 by binding to and inhibiting proteins in the cell that are needed for translation.
Plitidepsin is a similar molecule to ternatin-4 and is currently undergoing a clinical trial to treat COVID-19. The second drug, zotatifin, hits a different protein involved in translation. We are working with the CEO of the company that produces it to get it into clinical trials as soon as possible. The coronavirus attacks human cells using dozens of devious tricks. narvikk/iStock Getty Images Plus via Getty Images
The coronavirus attacks human cells using dozens of devious tricks. narvikk/iStock Getty Images Plus via Getty Images
Sigma receptors
The second group of drugs we identified work in an entirely different way.
Cell receptors are found both inside of and on the surface of all cells. They act like specialized switches. When a specific molecule binds to a specific receptor, this tells a cell to do a specific task. Viruses often use receptors to infect cells.
Our original map identified two promising MV cell receptors for drug treatments, SigmaR1 and SigmaR2. Testing confirmed our suspicions.
We identified seven drugs or molecules that interact with these receptors. Two antipsychotics, haloperidol and melperone, which are used to treat schizophrenia, showed antiviral activity against SARS-CoV-2. Two potent antihistamines, clemastine and cloperastine, also displayed antiviral activity, as did the compound PB28 and the female hormone progesterone.
Remember, all these interactions have so far only been observed in monkey cells in petri dishes.
At this time we do not know exactly how the viral proteins manipulate the SigmaR1 and SigmaR2 receptors. We think the virus uses these receptors to help make copies of itself, so decreasing their activity likely inhibits replication and reduces infection.
Interestingly, a seventh compound – an ingredient commonly found in cough suppressants, called dextromethorphan – does the opposite: Its presence helps the virus. When our partners tested infected cells with this compound, the virus was able to replicate more easily, and more cells died. Laboratory testing is excellent at generating leads but clinical trials must be done to know if these findings translate to the real world. Quantitative Biosciences Institute, CC BY-ND
Laboratory testing is excellent at generating leads but clinical trials must be done to know if these findings translate to the real world. Quantitative Biosciences Institute, CC BY-ND
This is potentially a very important finding, but, and I cannot stress this enough, more tests are needed to determine if cough syrup with this ingredient should be avoided by someone who has COVID-19.
All these findings, while exciting, need to undergo clinical trials before the FDA or anyone else should conclude whether to take or stop taking any of these drugs in response to COVID-19. Neither people nor policymakers nor media outlets should panic and jump to conclusions.
Another interesting thing to note is that hydroxychloroquine – the controversial drug that has shown mixed results in treating COVID-19 – also binds to the SigmaR1 and SigmaR2 receptors. But based on our experiments in both labs, we do not think hydroxychloroquine binds to them efficiently.
Researchers have long known that hydroxychloroquine easily binds to receptors in the heart and can cause damage. Because of these differences in binding tendencies, we don’t think hydroxychloroquine is a reliable treatment. Ongoing clinical trials should soon clarify these unknowns.
Treatment sooner rather than later
Our idea was that by better understanding how the coronavirus and human bodies interact, we could find treatments among the thousands of drugs and compounds that already exist.
Our idea worked. We not only found multiple drugs that might fight SARS-CoV-2, we learned how and why.
But that is not the only thing to be excited about. These same proteins that SARS-CoV-2 uses to infect and replicate in human cells and that are targeted by these drugs are also hijacked by related coronaviruses SARS-1 and MERS. So if any of these drugs do work, they will likely be effective against COVID-22, COVID-24 or any future iterations of COVID that may emerge.
Are these promising leads going to have any effect?
The next step is to test these drugs in human trials. We have already started this process and through these trials researchers will examine important factors such as dosage, toxicity and potential beneficial or harmful interactions within the context of COVID-19.
The 2005 regulations pushed on the World Health Organization by the United States and the Europeans hampered the WHO’s ability to declare an emergency and a pandemic.
BY VIJAY PRASHAD
http://inthesetimes.com/article/22492/world-health-organization-march-pandemic-covid-19
When U.S. President Donald Trump cut off his government’s funding to the World Health Organization (WHO), one of his grievances was that the WHO—under Chinese tutelage—failed to declare the global coronavirus outbreak as a pandemic soon enough. Not long after the virus brought patients to Hubei Provincial Hospital, the Chinese medical and public health authorities brought it to the notice of the WHO. The WHO investigated the virus over the course of early January, sending a team into Wuhan and making public whatever credible information it could report.
The WHO’s International Health Regulations (2005) Emergency Committee met twice in January, first on January 22-23 and then again on January 30; in the first meeting, the committee felt it had insufficient evidence to declare an emergency, but at the second meeting it took the decision to declare a public health emergency of international concern (PHEIC). This is the penultimate step for the WHO; on March 11, after it became clear that the virus was spreading across borders, but not before the WHO made many warnings to governments, the WHO declared a global pandemic.
Trump and his Democratic rival Joe Biden, as well as a host of other U.S. politicians, made the argument that the WHO did not act fast enough with its declaration. Whatever problems posed to the United States by the virus were not the responsibility of the U.S. government, they suggested; the fault lay with the Chinese government and with the WHO.
Our investigation finds that this argument has little foundation. The WHO’s reporting mechanisms are sound, but the WHO’s own ability to make these formal declarations—a public health emergency and a global pandemic, which come with serious financial consequences for member states—has been circumscribed; those who have constrained the World Health Organization—the United States and European nations—are the very same countries whose leaders are now complaining about Chinese influence over the WHO.
Revisions
By the 1990s, it had become clear that the WHO’s old International Health Regulations—originally issued in 1969, with only a few minor updates and new editions over the two decades after that—were inadequate. For one, these regulations were produced before the emergence of very infectious, lethal, and recurrent infections such as Ebola and the avian influenzas. Secondly, these old regulations were made before air travel began to move about 4.3 billion passengers per year, the scale of air traffic now making the movement of viruses so much easier.
In May 2005, the 58th World Health Assembly revised the 1969 regulations, pointing out that the new regulations would “prevent, protect against, control and provide a public health response to the international spread of disease in ways that are commensurate with and restricted to public health risks, and which avoid unnecessary interference with international traffic and trade.”
The North American and European states, in particular, insisted that the declaration of a PHEIC or global pandemic only be made after it was clear that air travel and trade would not be unduly interrupted. This restriction, essentially the core foundations of globalization, has constrained the WHO since 2005.
The 2009 Test
The new WHO regulations were tested when a new influenza emerged out of Mexico and the United States in mid-April 2009. This H1N1 was a combination of influenza virus genes that had links to swine-lineage H1N1 from both North America and Eurasia (thus the 2009 outbreak was commonly known as “swine flu”). It was first detected on April 15. On April 24, the U.S. Centers for Disease Control and Prevention uploaded a gene sequence onto a publicly accessible influenzas database. On April 25, ten days after the first detection of the virus, the WHO declared the 2009 H1N1 outbreak a PHEIC. On June 11, the WHO said that a global pandemic was underway.
In 2020, the WHO took a month to declare a PHEIC for the coronavirus and took an additional two months after that to pronounce a global pandemic. It was slower to announce the emergency, but it took the same time to declare a global pandemic.
By July 2009, the dangerous H1N1 virus had a less lethal impact than the WHO had feared. However, for the full year from its first detection, 60.8 million people were infected and 12,469 died.
Almost immediately, the WHO was attacked for the June 11 description of the outbreak as a pandemic. When the WHO declares a pandemic, governments are expected to do a variety of things including mass purchase of drugs and vaccines. These are costly.
That December, members of parliament in the Council of Europe opened an inquiry into the WHO declaration. Fourteen members of the Council charged the WHO with what was essentially fraud. They said that “pharmaceutical companies have influenced scientists and official agencies, responsible for public health standards, to alarm governments worldwide. They have made them squander tight health care resources for inefficient vaccine strategies and needlessly exposed millions of healthy people to the rise of unknown side-effects of insufficiently tested vaccines.” “The definition of an alarming pandemic,” they wrote, “must not be under the influence of drug-sellers.”
The criticism of the WHO stung. It had declared a pandemic, but the virus had stabilized very soon after the declaration. The WHO responded to such criticism with humility. “Adjusting public perceptions to suit a far less lethal virus has been problematic,” the WHO responded. “Given the discrepancy between what was expected and what has happened, a search for ulterior motives on the part of the WHO and its scientific advisers is understandable, though without justification.”
Trump’s Attacks
A WHO official told one of us that the agency had been shaken by the assault in 2009. Over the past ten years, the agency has struggled to regain its confidence, working through the Ebola outbreak in 2014 and then Zika in 2016. In neither of those cases was there a need to make any global declaration.
This year, the WHO declared a global pandemic within three months of the first cases. But there is no doubt that the attack on the WHO a decade ago has made an impact. Former WHO employees tell us that fear of being attacked like this by the main donors seriously hampers the independence of the WHO and its scientific advisers. Trump’s current attack is going to weaken further the ability of the WHO to operate at its own pace and with credibility.
The World Health Organization is not the first UN agency to face the wrath of the U.S. administration. The Trump administration sent its budget to Congress with zero dollars for a line item called International Organizations and Programs. Under this line item comes United States funds for UN Development Program, UNICEF, UNESCO, Office of the High Commissioner for Human Rights, UN Women, and UN Population Fund. In 2018, the United States stopped funding the UN’s Palestine agency (UNRWA). When the UN is useful, the United States uses it; when the UN goes against United States interests, it will lose its funding.
When Trump said that the WHO is “China centric,” he offered no evidence; he did not have to.
No doubt that the United States is currently facing the wrath of the global pandemic. If the U.S. government had begun to plan effectively after the WHO declared a public emergency on January 30 or even when it declared a global pandemic on March 11, the problems would not be so grave. But there was no planning at all, which is distressing. As George Packer put it in the Atlantic, the United States in the months after January was “like a country with shoddy infrastructure and a dysfunctional government whose leaders were too corrupt or stupid to head off mass suffering.” From Trump, the U.S. citizenry got “willful blindness, scapegoating, boasts, and lies.” This sums it up. Part of the scapegoating was directed at China; it is far easier to blame China—already part of a dangerous trade war and a simmering regional struggle in Asia—than to accept responsibility oneself.
(This is the second part of a two-part series, which is fully available here.)
I’m a mother of 6-year-old twins and like millions of other Americans, I can’t pay rent—so I’m going on a rent strike.
BY JENAY MANLEY
http://inthesetimes.com/article/22496/congress-cancel-rent-may-day-homes-guarantee
Rent is due tomorrow, and I—like millions of other Americans—am not going to be able to pay.
I work overnights as an “essential worker” at a gas station. My shift starts at 10pm and ends at 7am. And I’m a mother of 6-year-old twins. The Covid-19 crisis has thrown our future into chaos. I am working 46 hours a week, getting home just before my two children wake up and trying to help them navigate multiple online platforms to keep up on their homework.
About six months ago, I asked my kids’ father to move back in with us so that I could afford rent. The relationship turned toxic again very quickly. I needed him to leave, and I finally got him out in late March. But that has meant that the person who was supposed to be watching my children is no longer around. On April 1, I had to scramble to come up with his portion of the rent. Even after donating my own plasma and using savings, I couldn't do it without help.
I am lucky to still have work right now, but that work comes with extreme stress during this crisis. I am filled with anxiety about catching the virus, as I am exposed to up to 200 people a night while working, and I'm facing huge financial losses due to the cost of childcare. My great-aunt who usually watches my kids when I am in a pinch is in her late 60s. She is at extremely high risk for contracting Covid-19 and has struggled with her health for years.
I’m not sleeping. I’m exhausted. And I'm getting desperate. I couldn't make April's rent without help, and I will barely be able to make rent this week on May 1. By no fault of my own, I'm being driven to the brink of total crisis. How does this country and all of its lawmakers let this happen to people?
I'm not alone in my struggle. Nearly a third of all U.S. renters couldn't pay on April 1. Over 30 million Americans have filed for unemployment since the pandemic began. And still more, like me, are working but financially strapped due to the crisis. This week, millions more won't be able to pay the rent. Those who do pay will be forced to make decisions between rent and food, or their medications and their housing.
When I’m not working or caring for my kids, I also organize as a leader with the housing justice group KC Tenants in Kansas City, MO. I also work with the grassroots organization People's Action on the campaign for a national Homes Guarantee. We’re not just fighting for immediate relief. We’re fighting for a different world, in which housing is guaranteed as a human right.
I’ve been living in crisis long before the pandemic took hold. Even before Covid-19 spread to the United States, more than 10 million people were spending over half their income on a rent check to their landlords. I'm always one emergency away from eviction or homelessness, among the 40% of Americans who don’t even have $400 in the bank. Capitalism and racism have built a broken, oppressive, extractive housing system that has always failed myself and other working-class people. Now, we're just seeing that failure more clearly.
As I see it, members of Congress have two choices: 1) come to Kansas City and babysit my kids while I'm at work or 2) cancel rents and mortgage payments in the next stimulus package. Our representatives will have a chance to negotiate for relief in the next stimulus, thanks to a recent bill introduced by Rep. Ilhan Omar, the Rent and Mortgage Cancellation Act.
We need a real bailout for the people, and rent and mortgage cancellation must be part of it. Today, I'll be taking this struggle to the streets in Missouri, bringing our state’s crisis to the person with the power to solve it, our Governor Mike Parson. And I'll be identifying as a rent striker, politicizing my inability to pay the rent and calling on the government to step up and do something about it.
The Foundation for Defense of Democracies and American Enterprise Institute are aggressively campaigning for military escalation and a tightening of sanctions.
BY SARAH LAZARE
http://inthesetimes.com/article/22487/think-tanks-fdd-aei-iran-sanctions-coronavirus-war-trump-pompeo-covid
Since the global Covid-19 pandemic began, a cluster of U.S. think tanks has been aggressively lobbying the Trump administration to escalate militarily toward Iran and tighten U.S. sanctions. This push has come despite warnings that such sanctions are worsening the death toll of Iran’s outbreak, which is one of the worst in the world. The think tanks leading this effort—the Foundation for Defense of Democracies (FDD) and American Enterprise Institute (AEI)—have cranked out non-stop statements, research documents, videos and media appearances since the crisis began. They are not shouting into the wind, but speaking directly to an administration that has proven willing to act upon their words.
In the 47 days since March 11, when the World Health Organization declared Covid-19 a global pandemic, the FDD has posted 56 articles, podcast interviews and videos on its website which either demonize Iran as a uniquely bad actor or urge the United States to take a confrontational posture towards the country. While the steady stream of anti-Iran invectives is not new, the insistence that the Covid-19 crisis builds their case is. One piece from April 14, for example, argues that the crisis strengthens the case for “regime change,” because it will diminish “the regime’s credibility even further and add fuel to the outrage and anger that have been building for years.” The unproven theory that mass suffering will accelerate an uprising against the government has long been used to justify a host of punishing U.S. policies against the Iranian people, including sanctions—a form of collective punishment has only unleashed poverty and premature death upon ordinary people.
Yet, throughout the crisis, the FDD has published a flurry of materials arguing that the United States must not let up sanctions during the pandemic. The organization is funded by pro-Israel billionaires and started out in 2001 as an explicitly pro-Israel organization called EMET (Hebrew for truth). Since the pandemic began, it has published written and video posts that include: “Tehran Can Afford to Fight Covid-19 Even Without Sanctions Relief,” “The Coronavirus Is Absolutely No Excuse To Lift Sanctions on Iran” and “Humanitarian channels to Iran continue to be wide open.” In a March 27 video, Mark Dubowitz, the chief executive of FDD, released a video arguing that “the Iranian people know that this is the wrong time to give sanctions relief.”
In fact, doctors in Iran have been begging the Trump administration for relief from sanctions, which are cutting off critical medical supplies, like ventilators, leading to an increase in Covid-19 deaths. While humanitarian exemptions technically exist on paper, they are rendered largely meaningless by a difficult-to-navigate web of sanctions, as well as threats and intimidation from the Trump administration, which have scared global banks and firms from doing business with Iran. Researchers were warning that sanctions were causing a shortage in medical supplies before the outbreak began: As Human Rights Watch said on April 6, “these exemptions have failed to offset the strong reluctance of U.S. and European companies and banks to risk incurring sanctions and legal action by exporting or financing exempted humanitarian goods.”
Hoda Katebi, an Iranian-American community organizer with the No War Campaign, told In These Times that the FDD’s role is “wildly ruinous—there's no nicer way to put it.” According to Katebi, “You'd think a humanitarian crisis would be a time when war hawks pause rather than ramp up their project. It is telling what their goal is. With all their talk about wanting to help the Iranain people, it’s very clear it's quite the contrary.”
Amid calls for sanctions relief, the Trump administration has only dug in more, with Secretary of State Mike Pompeo issuing a statement on March 18 announcing a new round of sanctions that “will deprive the regime of critical income from its petrochemical industry and further Iran’s economic and diplomatic isolation.” This was soon followed by the Trump administration’s intervention to block an emergency $5 billion loan to Iran from the International Monetary Fund (a position the FDD also supported). But this did not satisfy the FDD. On April 23, a group of “experts and formal officials” signed a letter to Trump urging his administration to “double down on the maximum pressure campaign.” Of the 50 people who signed, 22 were from the FDD, according to a report in the conservative publication The National Interest.
Cavan Kharrazian, international program researcher for the Center for Economic and Policy Research, told In These Times, “Their letter echoes the State Department's categorically false line that these broad economic sanctions have no humanitarian effects. Despite claiming that their ‘hearts go out’ to the Iranian people, they actively contribute to an extremely dangerous foreign policy that harms millions of ordinary Iranians and pushes us closer to escalating military conflict.” This danger is underscored by Trump’s April 22 claim that, “I have instructed the United States Navy to shoot down and destroy any and all Iranian gunboats if they harass our ships at sea”—a reference to the U.S. Navy's Fifth Fleet in the Persian Gulf.
One of the signatories is the FDD’s senior advisor Richard Goldberg, who worked in the Trump administration from 2019 to 2020 while he was also at the FDD. When serving as Trump’s national security advisor, John Bolton created a job just for Goldberg: “director for countering Iran’s weapons of mass destruction.” As Bloomberg reports, “The goal was to counter what Bolton saw as a desire at the departments of State and Treasury to weaken the ‘maximum pressure’ campaign against Iran.” While Goldberg served on the National Security Council, he remained on the salary of the FDD.
Goldberg’s double role is not the only evidence of a close relationship between the FDD and the Trump administration. When Iran declared in August 2019 that it was imposing sanctions on the FDD and Dubowitz for “unilateral and illegal economic terrorism,” Pompeo came to the think tank’s defense. “The U.S. does not take these threats lightly, and will hold the regime and its ‘apparatuses’ to account,” he tweeted. On April 17, Juan Zarate, Chairman of the FDD’s “Center on Economic and Financial Power,” appeared on a roundtable, organized by the Center for a New American Security (CNAS), alongside Andrea Gacki, director of the Office of Foreign Assets Control for the U.S. Department of the Treasury, where he argued in favor of U.S. sanctions. Among the FDD’s biggest funders is billionaire and Home Depot co-founder Bernard Marcus, who was one of Trump’s largest donors in 2016 and has been clear about his fervent belief that “Iran is the devil,” as Eli Clifton reported.
According to Kharrazian, “In the realm of public opinion, FDD CEO Mark Dubowitz is continually quoted in major publication pieces on Iran, such as the New York Times, and FDD staff members routinely host or sit on panels throughout the beltway regarding Iran. Additionally, their 'experts' have regularly testified in Congress on foreign policy towards Iran.”
But perhaps the clearest sign of influence is how closely the Trump administration’s rhetoric mirrors that of the FDD. On April 6, the State Department published a fact sheet titled “Iran's Sanctions Relief Scam.” This bizarre, screedy document is worth comparing with an FDD memo published the day before: the overlap in messaging, historical examples, and specific data cited is striking. As Kharrazian notes, this is not an isolated case: “If you read the statements coming from Trump's State Department on Iran and the 'maximum pressure' campaign, they appear almost completely ideologically aligned with these think-tanks' own positions and talking points, especially during the Covid-19 crisis.”
FDD is not alone in its campaign. The AEI, which has received millions from Koch foundations, as well as corporations such as ExxonMobil, has launched a campaign to counter activists who are calling for sanctions relief. Yasmine Taeb, senior policy counsel at Demand Progress, tells In These Times, “FDD and AEI have always pushed for policies aimed at war. FDD led the charge against the Iran nuclear deal under Obama, and it opposes U.S. diplomacy with Iran on principle: It sees any U.S. relationship with Iran as coming at the expense of the U.S. relationship with Israel, and it has a track record of supporting escalation for the sake of escalation.”
“The difference between the FDD and AEI today is that the AEI is a prominent conservative organization that supported Bush’s march to war in Iraq in 2003,” she continues. “It is not leading the charge for war with Iran today: The FDD is playing the role that the AEI played in the lead-up to the Iraq War.” Notably, AEI’s board of trustees includes former Vice President Dick Cheney alongside and a number of corporate leaders, including Christopher B. Galvin, former CEO and chairman of Motorola.
While the AEI might not be playing as large a role as the FDD, it also is not silent. On March 20, 26 progressive organizations released a statement asking “President Trump, Sec. Mnuchin, and Sec. Pompeo to loosen the administration's crippling sanctions regime on Iran for 120 days in order to aid the Iranian people’s fight against the virus.” AEI responded with a press effort to oppose that effort. On March 24, AEI resident scholar Michael Rubin directly blasted the letter in an op-ed in the Washington Examiner titled, “Don’t lift Iran sanctions, not even for the coronavirus.”
Then, on March 25, AEI senior fellow Danielle Pletka wrote an op-ed in The Dispatch titled, “Sorry, now is not the time to lift sanctions on Iran.” That piece also responds to the letter from 26 organizations calling for sanctions to be lifted. In late March, Sen. Bernie Sanders, Reps. Alexandria Ocasio-Cortez and Ilhan Omar and others circulated a letter calling for immediate sanctions relief for Iran (that letter would be publicly released on March 31 with 34 congressional signatures). On March 25, Rubin wrote an article for The National Interest titled “Sorry, AOC: Donald Trump can’t give Iran a sanctions pass for coronavirus.”
Nahid Soltanzadeh is a digital campaigner for the Muslim grassroots organization MPower Change, which is part of the #EndCOVIDSanctions coalition that released a March 31 letter applauding those members of Congress who spoke out against U.S. sanctions. They said that the push by both the AEI and FDD to increase sanctions “is enraging and only enables the Office of Foreign Assets Control to continue letting Iranians die from Covid-19.” Soltanzadeh underscored, “They create an environment where OFAC can escape accountability to the U.S. public or Congress—both of which are overwhelmingly demanding a temporary lift on Iran sanctions.”
Katebi says the AEI’s campaign is a sign of the effectiveness of sanctions opponents: “For them to be going so strong, it's only because they're seeing the work and impact we've been having as a campaign.”
Like the FDD, AEI’s support for sanctions stems from a larger push towards military escalation. On April 10, Gary Schmitt, “resident scholar in strategic studies and American institutions” for AEI, wrote a piece in The American Interest titled, “Don’t slash the defense budget to pay for Covid-19.” He argued that any cuts would pose a security threat to the United States, in part because “Russia, China, and Iran have become more aggressive and more potent adversaries.” On April 2, Kenneth M. Pollack, a resident scholar at AEI, echoed FDD in speculating on whether the mass suffering caused by Covid-19 could hasten the regime’s end: “While Covid-19 seems unlikely to be the trigger for the fall of the Islamic Republic, when the regime’s history is finally written, it may very well be that we will look back on this crisis and say that it helped hasten its end.” Notably, Pollack was a major pusher of the Iraq war, who was cited by New York Times columnist Bill Keller as a reason the latter supported that war.
Meanwhile, some at AEI are making the case that “bad actors” like Iran will try to take advantage of the crisis, so the United States should too. Hal Brands, resident scholar for AEI, wrote an article for Bloomberg opinion on April 20 titled, “The world’s bad actors see coronavirus as an opportunity.” He wrote, “There will always be predatory actors looking to exploit weakness and disorder, even if that disorder affects them as well. If the guardians of order are absent, the balance will be broken, and the results will not be pretty.”
Amid an unprecedented global crisis, the self-declared “guardians of order” see an opening to push for more war, death and destruction. In the words of Taeb from Demand Progress, “It's pretty disgusting, because we're talking about a global pandemic that has claimed the lives of hundreds of thousands of people. We're talking about innocent people dying.”
To safely reopen the economy, we need a public health corps. Here’s how to build it.
BY DAYTON MARTINDALE
http://inthesetimes.com/article/22493/contact-tracing-jobs-corps-covid-coronavirus-testing-congress-stimulus
As of last Thursday, 26.5 million Americans had filed for unemployment in a five-week span, as businesses not deemed essential are scaling back or shuttering entirely. Yet perhaps the most essential work of all remains stubbornly undone.
To safely reopen the economy without new waves of infection and death, virtually everyone who has written on the topic has been repeating the same urgent recommendation for months: The United States must ramp up testing, and with it employ a robust program of “contact tracing.” That is, we must reach out to those who test positive, determine who they have been in close contact with, alert these contacts that they may have been exposed, and ensure that these contacts are able to effectively quarantine. While technological tools play a role in this, providing personalized support will take people power.
In response, several cities and states have begun bringing on paid staff and volunteers for tracing, but these local actions are far from the scale needed. Experts suggest the United States will need a bare minimum of 100,000 to perform this task, while former Centers for Disease Control and Prevention (CDC) director Tom Frieden has suggested as many as 300,000. And this is only one of many pandemic-related tasks for which our badly understaffed public health system needs new recruits and fast.
In short, we face two interrelated problems: More people than ever are newly out of a job, and the government needs to rapidly expand its own workforce. The solution may seem obvious, and indeed a wide range of actors have called for federal hiring programs.
Unfortunately, Congress has thus far seemed more concerned with bailing out big business than with public health or unemployment. But recent proposals from a working group of Senate Democrats—and even, on Monday, from Joe Biden—suggest that there may be increased momentum behind something like a New Deal-era federal jobs program: a large civilian corps of public health workers hired primarily from the ranks of the unemployed. There’s no reason to wait: The next coronavirus bill should include funding for hundreds of thousands of public health jobs, including an explicit provision for 300,000 full-time, salaried contact tracers, managed by the CDC, to be recruited, trained and hired as soon as possible.
Where we’re at
Thus far, cities and states have taken the lead in contact tracing. Massachusetts has allied with the nonprofit Partners in Health to commit to employing 1,000 tracers (and received more than 15,000 applications). Washington state, which currently has 700 tracers, intends to reach 1,500 by the second week of May. In California, Gov. Gavin Newsom announced his intent to train a statewide tracing workforce of 10,000.
These efforts represent important steps forward, but they are not enough. For one, they’re too small: Univeristy of California San Francisco infectious disease expert George Rutherford estimated California might need three to four times that number.
Just as importantly, their patchwork nature is inadequate to addressing a crisis that doesn’t neatly respect state and county borders. According to Leif Wellington Haase, health policy consultant and former director of The Century Foundation’s Public Health Preparedness and Bioterrorism Project, while wealthier economies like California’s might be able to set up large-scale contact tracing, “There are lots of places in the country, especially in rural areas, where no one will set up contact tracing and there’ll be no impetus to set it up until it’s much too late.” A nationwide program could coordinate priorities, establish standardized protocol and reach otherwise neglected communities.
There’s one more big reason you need a national program: funding. States are unable to print their own money as the federal government can, and almost all are required to balance their budgets. Even if they do set aside funds for hiring contact tracers, this may come at the expense of cuts elsewhere—indeed, cuts have already begun. Some states are relying partly on volunteers, presumably to save money, but this is a missed opportunity when so many desperately need paid work. Plus, Haase adds, “unless you pay people you’re not going to have the first-rate, consistent, well-trained workforce that you ultimately need.”
The most recent federal coronavirus bill, signed into law April 24, does allocate $25 billion toward developing and implementing testing and related expenses, including contact tracing. While this is a respectable chunk of money, testing is expensive and will likely require the lion’s share of the funds.
One estimate from the Rockefeller Foundation suggested a scaled-up testing effort could cost $100 billion in the short term, and up to $500 billion over the next year. (Administering these tests could be another job for new public health workers.) While this estimate is on the high end, it’s clear that the nation’s public health infrastructure—whose per capita funding decreased 9% from 2008 to 2016, and which has been gutted further under Trump—is going to need more resources. Adequate testing enables tracing to be more comprehensive, but we can’t just neglect the latter: A federal jobs program for contact tracing will require its own dedicated funds.
What we need
The good news is that contact tracing is relatively cheap. Experts estimate that a full fleet of 300,000 would cost in the range of $10 to $15 billion, primarily in labor costs, depending on pay and benefits for workers. Pay proposals from various academics and think tanks range from $17 an hour to $50,000 plus benefits—let’s push for the latter, because even $15 billion is a tiny fraction of the trillions already spent an economic relief.
On April 22, one day after the Senate passed the latest relief bill, a working group of Senate Democrats released two proposals to ramp up hiring for federal public health. A third is reportedly on the way.
The first suggests a dramatic expansion of AmeriCorps and other national service programs—doubling to 150,000 workers in the next year, and 300,000 in each of the two years after—meant to perform not only public health tasks but education support and other needed services. (Expanding existing service corps is also the idea behind Biden’s newly proposed “U.S. Public Health Jobs Corps” for contact tracing, though the presumptive nominee did not flesh out many details.) Indeed, several AmeriCorps organizations are already doing pandemic-related work, such as mask-making and meal distribution; the bill would make this the norm across the entire network and ramp up capacity. The proposed legislation also sets up a new partnership between the CDC and AmeriCorps, creating a CDC Corps that could theoretically carry out contact tracing.
“Scaling up existing systems … can be helpful when you need to move fast,” says Daniel Edelman, associate director of strategy and operations at the policy think tank Next100 and co-author of that group’s recent report, “The Road to COVID-19 Recovery Is Long—But AmeriCorps Can Help.” Edelman underscores, “AmeriCorps has historically had bipartisan support, so it might be a good vehicle.”
One area where the plan might improve is pay: The bill does permanently increase AmeriCorps compensation to 175% of the federal poverty line—a significant boost over its current low rate, but, at $22,330 for a one-person household, far from a fair wage. An earlier bill from Sens. Ed Markey (D-Mass.) and Chris Van Hollen (D-Md.)—who also support the new proposal—had suggested 200% of the poverty line, and progressives should demand even more, including the right of participants to unionize.
In the second Senate proposal, introduced by Sens. Kirsten Gillibrand (D-N.Y.) and Michael Bennet (D-Colo.), the federal government would hire hundreds of thousands of workers for a new “Health Force.” This force would be managed by state and local agencies who best know what their communities need, but directed and coordinated by the CDC.
This health force would engage in everything from tracing contacts to administering tests to delivering food to the old, sick and immunocompromised.
This second proposal may be the most promising path toward a well-paid, full-scale contact tracing corps, as it is not constrained by AmeriCorps’ pay issues and leaves room for a greater number of workers (though the first can still play a complementary role).
The Senate Democrats in this working group have explicitly evoked the 1930s Works Progress Administration (WPA) and Civilian Conservation Corps (CCC) as models. These New Deal precedents show that government jobs programs can be popular not only among those who are employed, but among the community writ large, which benefits from the work itself as well as the broader economic boost.
This history also shows that jobs programs can get off the ground quickly. President Roosevelt pitched the CCC to Congress on March 21, 1933, and by late April, “they raised the first flag in the first CCC camp in the nation,” says Neil M. Maher, history professor at the New Jersey Institute of Technology and author of Nature’s New Deal: The Civilian Conservation Corps and the Roots of the American Environmental Movement. Part of what streamlined this process is that the CCC drew on existing government agencies to coordinate, rather than launching something new out of whole cloth.
A public health corps could do likewise. “The CDC absolutely has the internal knowledge and capacity to run something like this,” Haase says. Such a corps, he estimates, could be put together in about two months, assuming a competent and well-intentioned government. While that’s a big “if” in the current administration, contact tracing is a relatively easy job to train for—it primarily requires people skills and access to a phone, rather than any public health background or even a college degree. Laid-off workers from a wide range of backgrounds could participate. In Massachusetts, tracers who trained on a Thursday were making their first calls by the weekend.
The path forward
Perhaps the biggest obstacle to a federal public health corps is Mitch McConnell. So far, coronavirus relief bills, originating in the senate, have fallen short of protecting everyday working people; the most recent bill garnered the opposition of Rep. Alexandria Ocasio-Cortez (D-N.Y.) as well as several progressive groups including People’s Action, Sunrise and Indivisible. And the House, says Indivisible national policy director Angel Padilla, “is swallowing whatever the Senate gives it.”
For this reason, Padilla hopes the next bill—which could come this week, he says—will be drafted first in the House rather than the Senate, giving Democrats more control over what’s in it.
If this is the case, House Democrats might use one or both of the Senate Democrat proposals as a launching point, making a public health corps a key component of any relief program. They could flesh out the details to ensure a genuinely progressive result, with high pay and benefits, priority given to the jobless and marginalized, and, crucially, guarantees of privacy and data security.
Senator Markey has sent multiple letters to the Trump administration raising concerns about the potential for contact tracing technologies to violate civil liberties. Partnering with private entities will be necessary, he concedes—and has already begun, with several tech companies and even Michael Bloomberg all developing programs—but individuals’ information sharing must be voluntary. In addition, public and private actors must be fully transparent about what data they are collecting, why, and what it can be used for, with strict legal protections prohibiting access to any personal health information.
For all this to happen, Congress will likely need a push. So far, relatively little federal-level activism has prioritized testing and tracing. Understandably, community organizations and progressive politicians are focused on putting out the economic fires first—providing unemployment insurance and rent relief, for instance—which can feel more urgent and fits better within groups’ existing priorities and expertise. “Public health in and of itself is not really the main concern of federal politicians,” Haase says.
But in the long game, testing and tracing are essential to maintaining lives and livelihoods, and progressives should start pressuring their congresspeople to support a Health Force now. While conventional protests are now unsafe, organizers continue to send calls, emails, videos and tweets at legislators—there is anecdotal evidence politicians are replying to tweets more often, Padilla says—and other organizations are experimenting with creative new tactics. Members of unions and community organizations that are already organizing around COVID-19 relief can petition within their groups to add a public health corps to their list of demands.
McConnell is unlikely to be on board: He initially signaled that he thinks states should be able to take care of themselves (though he walked this back on Monday), and is in no rush to pass the next bill. Moving forward, then, it may be even tougher to wring concessions out of the Senate GOP.
But this “let-states-fend-for-themselves” strategy, which is already falling short, may contain the seeds of its own downfall. The decentralized approach reminds Maher of President Hoover’s posture toward the Great Depression—let local, state and private actors deal with it. This failed dramatically, priming Americans to support Roosevelt’s more active approach. Perhaps, as people watch the virus devastate their communities, McConnell’s failure will spur a similar shift.
There is evidence a public health corps could be popular. A similar proposal for a “Climate Conservation Corps” oriented around green jobs has 61% support and only 21% opposition, and polls show most Americans take the virus seriously. “I don’t think that people realize how angry the base is,” Padilla says.
Some of the experts In These Times spoke to suggest that, strategically, a public health corps is more likely to get through Congress framed as a temporary crisis response. But all of them underlined that the need for more public health workers does not end in a crisis. “The problem is when we think about these policies as crisis policies, that guarantees that they will be closed down as soon as people perceive that the crisis is gone,” says Pavlina Tcherneva, associate professor of economics at Bard College and the author of forthcoming book The Case for a Job Guarantee. “The pandemic will go away but the existential problems”—in the economy writ large and in our underfunded public health infrastructure—“will not go away.”
In fact, a permanent public health corps—or better yet, Tcherneva suggests, a full job guarantee—would make us far more prepared for the next crisis, be it another pandemic or some climate catastrophe. Had we had such a corps two months ago, we could have expanded contact tracing much more quickly smoothly. Many jobs that might now be considered pandemic response—child care for health workers, support for the elderly, food distribution—are needs that exist even in normal times, and a public health force might also be redirected to green jobs, as climate change, habitat destruction and pollution contribute to everything from infectious disease to cancer. A full jobs guarantee, Tcherneva says, would enable anyone to get a paycheck for making a valuable contribution to society, whether that’s putting up solar panels or, this spring, just staying home.
A federal jobs guarantee might seem unlikely to pass a McConnell Senate, but much that once felt unlikely is suddenly on the table. The support for mass hiring for public health by moderates like Biden, Michael Bennet and Amy Klobuchar suggest that some surprising faces may be open to New Deal-style programs—even if the Left will have to turn up the heat to make sure these programs are sufficiently robust.
We now have the opportunity to provide people well paying, meaningful work that genuinely helps the larger community, as we did in the 1930s. Or we can keep watching the virus eat away at our social and individual immune systems, causing the economy—and human bodies—to break down. The choice is straightforward: indefinite shutdown, mass death, or a federal public health corps.
 Every place that a coronavirus protein interacts with a human protein is a potential druggable site. QBI Coronavirus Research Group, CC BY-ND
Every place that a coronavirus protein interacts with a human protein is a potential druggable site. QBI Coronavirus Research Group, CC BY-ND With dozens of drugs each needing full testing, to get results in four weeks required round-the-clock effort. Quantitative Biosciences Institute, CC BY-ND
With dozens of drugs each needing full testing, to get results in four weeks required round-the-clock effort. Quantitative Biosciences Institute, CC BY-ND The coronavirus attacks human cells using dozens of devious tricks. narvikk/iStock Getty Images Plus via Getty Images
The coronavirus attacks human cells using dozens of devious tricks. narvikk/iStock Getty Images Plus via Getty Images Laboratory testing is excellent at generating leads but clinical trials must be done to know if these findings translate to the real world. Quantitative Biosciences Institute, CC BY-ND
Laboratory testing is excellent at generating leads but clinical trials must be done to know if these findings translate to the real world. Quantitative Biosciences Institute, CC BY-ND