Monday, May 4, 2020
To know the real number of coronavirus cases in the US, China, or Italy, researchers say multiply by 10
https://www.businessinsider.com/real-number-of-coronavirus-cases-underreported-us-china-italy-2020-4
The world may never know the full extent of the coronavirus pandemic.
Researchers agree that the true number of COVID-19 cases is much larger than official global tally — particularly in nations with severe outbreaks like China, Italy, and the US.
In these countries, limited testing capacity and the difficulty of finding and identifying asymptomatic cases has likely caused many patients to go undiagnosed. COVID-19 tests can also produce false negatives if they aren't administered properly or if a patient isn't shedding enough virus to be detected in a sample.
Some public-health experts have suggested that the actual case totals in China, Italy, and the US could be at least 10 times higher than the current figures.
"Really nobody knows," Elizabeth Halloran, a biostatistician at Fred Hutchinson Cancer Research Center and University of Washington, told Business Insider. "A lot of people have been missed."
National outbreaks could be much larger than data suggests
Halloran said the actual number of US cases could be anywhere from 5 to 20 times the current number, based on recent models. But any model, she added, should be taken with a grain of salt.
Many coronavirus models are based on back calculations that try to determine how many people were infected several weeks ago. Researchers then extrapolate these findings to estimate the present number of cases.
So far, these methods have indicated that China, Italy, and the US are all underreporting cases by a similar order of magnitude.
Neil Ferguson, a professor of epidemiology at Imperial College London, estimated in February that China had only detected around 10% or less of its coronavirus cases.
Similarly, the head of Italy's Civil Protection Agency told the newspaper La Repubblica in March that it was "credible" to assume a ratio of one confirmed case for every 10 infections in Italy.
Trevor Bedford, an epidemiologist at Fred Hutchinson, estimated last weekend that the US was confirming between one in 10 and one in 20 infections. That would put the actual case count at around 5 million to 10 million.
A March study in the journal Science suggested that the US outbreak was five to 10 times larger than the reported number.
"A lot of the models take different methods and converge on the same results," Halloran said, though she added that "there is a lot of uncertainty."
Identifying asymptomatic patients would raise the case count
One of the biggest hurdles to getting accurate coronavirus case counts is the fact that infected people can be asymptomatic.
"We don't know how many asymptomatic infections there are," Halloran said. "Those people, we suspect, are a source of a lot of the transmission in the population."
Anthony Fauci, director of the National Institute of Allergy and Infectious Disease, recently estimated that between 25% and 50% of people infected with the coronavirus may never show symptoms but can still be contagious.
Some estimates are even higher. A study of 3,000 people in Vo'Euganeo, a village in northern Italy, found that between 50% and 75% of coronavirus patients there were asymptomatic. In a letter to Italian authorities in Tuscany, Sergio Romagnani, a professor of clinical immunology at the University of Florence, said that asymptomatic patients represent a "formidable source of contagion."
A February report from the World Health Organization found that asymptomatic cases were "relatively rare" in China, but the country's National Health Commission later determined that 78% of new infections reported on April 1 were asymptomatic. This suggests patterns from China's early data may not be reliable or widely applicable.
Testing errors and limited testing capacity obscure the reality of the pandemic
The more tests get administered, the more countries are likely to identify cases. But many nations are still struggling to provide enough tests for prospective patients. Even in Italy, which has one-fifth the population of the US and 23 times fewer people than China, tests aren't accessible to all residents.
Though Italy initially offered widespread testing, including tests for patients without any symptoms, the nation's current policy is to only test people with severe symptoms.
At the height of China's outbreak, the country also reserved tests for people who were sick enough to show up at a hospital. Since tests were initially in short supply and took days to process, Chinese doctors briefly resorted to diagnosing patients in the Hubei province via CT scans. Colin Furness, an infection control epidemiologist at the University of Toronto, told ProPublica that medics in China also started diagnosing patients based on symptoms alone.
In New York City, the epicenter of the US outbreak, hospitals are still limiting testing to patients with severe illnesses. States with major outbreaks like California and Washington have also reported a backlog in test processing and shortages of materials like swabs.
What's more, tests can be faulty. A study of more than 1,000 hospital patients in Wuhan, China, found that 75% of people whose tests came back negative likely had COVID-19 based on their CT scans.
"There are a lot of things that impact whether or not the test actually picks up the virus," Priya Sampathkumar, an infectious-diseases specialist at the Mayo Clinic, told AFP. "It depends on how much virus the person is shedding (through sneezing, coughing and other bodily functions), how the test was collected, and whether it was done appropriately by someone used to collecting these swabs, and then how long it sat in transport."
Together, these limitations contribute to a vast underreporting of cases.
Tests for current patients "need to be faster and cheaper and more reliable and available in much greater quantities," Halloran said.
Blood tests could identify more cases, but some deaths will never be counted
Public-health experts are still debating the death toll of the 1918 Spanish flu more than a century later. Some estimate that around 20 million people perished, while others believe the death count reached 100 million.
Halloran said the current pandemic will be easier to understand, since researchers will eventually be able to use a blood test to determine whether people have developed antibodies to the virus.
"We'll have to piece it together with serology afterwards," she said. "There could be a lot more people infected than we thought."
But antibody testing would have to be rolled out on a giant scale to give researchers a firm understanding of the scope of the pandemic.
"You could go around and test people that are going back to work or go out in the neighborhood or look at healthcare workers — how many of them actually had the infection and never knew it," Halloran said. "That's what we need to do to understand how widely people have been infected."
Even then, she added, there will always be some cases that are never identified.
Between March 4 and April 4, New York City reported more than twice the typical number of monthly deaths, according to the New York Times. Of the 5,330 excess deaths recorded during that month, only 3,350 were confirmed coronavirus deaths.
"We won't ever know if those 2,000 deaths were coronavirus deaths or from something else," Halloran said. "It's a single city in a single month where they probably have a two-week delay in reporting deaths. Probably the number is much greater."
U.S. CORONAVIRUS DEATH TOLL MAY ONLY BE 'TIP OF THE ICEBERG,' SAYS CDC ADVISORY COUNCIL MEMBER
BY SOO KIM
ON 4/16/20 AT 1:00 PM EDT
https://www.newsweek.com/us-coronavirus-death-toll-may-only-tip-iceberg-says-cdc-advisory-council-member-1498352
As the COVID-19 pandemic continues across the U.S., obtaining an accurate tally of cases and deaths has become a growing challenge.
Death counts may be underestimated due to several factors. Staff shortages and bureaucratic red tape around accessing death records in certain states have also reportedly added to the issue, causing delays in reporting the latest state figures to the U.S. Centers for Disease Control and Prevention (CDC).
But many potentially infected people have been dying at home. These deaths are currently unaccounted for because of a lack of testing before they died.
Several metropolitan areas of states with some of the highest death tolls in the country have reportedly seen a spike in fatalities at home that may have been from COVID-19.
Speaking to Newsweek, Mark Hayward, an expert on mortality statistics who is a member of a CDC advisory council on vital statistics, said: "The biggest challenge in obtaining an accurate tally of COVID-19 deaths is to [be able to] implement widespread testing. Locales that lack testing and where populations are rural, reside in nursing homes, or people live alone are likely to be major contributors to the undercount; note that these are not mutually exclusive categories."
He added: "There are also varying standards (and timing of rollouts) of testing by state. Cause-of death classification schemes have also been evolving and it's not always straightforward in assigning COVID-19 as a cause of death. I think the biggest barrier, though, is the lack of testing."
As of Thursday, nearly 3,263,000 people in the U.S. have been tested for the virus. This is less than 1 percent of the total population.
So the current reported U.S. death toll may only be "the tip of the iceberg," Hayward told ProPublica.
But just how underreported are the death counts across the U.S.? Hayward told Newsweek: "I do not have an actual figure of underreporting and this will vary over time as testing becomes more widespread. The degree of under-reporting will vary across localities in the U.S. and over time. The geographic and temporal variability are tightly linked because of the geographic differences in testing."
He added: "It's also hard to use other countries as standards to gauge underreporting, given differences in vital registration systems."
Getting an accurate account of deaths is vital for mitigation purposes, especially for identifying any potential hotspots and sending resources to those areas before there is an explosion of cases and deaths. That's according to the chief of the CDC's mortality statistics branch, Robert Anderson.
"One of the reasons we count deaths is to allocate resources to where they need to go. It becomes a little more time-sensitive when you're dealing with something like a pandemic," Anderson told ProPublica.
New York City, the country's most populous city with nearly 8.4 million residents, reported around 200 people a day were dying at home, a spokesperson for the medical examiner's office, Aja Worthy-Davis, told Gothamist last week.
An untold number of deaths were said to have been unconfirmed and the medical examiner's office does not test dead bodies for the virus.
A spokesperson for the city's health department, Michael Lanza, told Gothamist that the city only includes confirmed novel coronavirus deaths in official figures. "Every person with a lab-confirmed COVID-19 diagnosis is counted in the number of fatalities," he said.
"While undiagnosed cases that result in at-home deaths are connected to a public health pandemic...not all suspected COVID-19 deaths are brought in for examination by OCME [Office of Chief Medical Examiner], nor do we provide testing in most of these natural at-home deaths."
Nearly 2,192 deaths at home (equating to about 130 deaths a day) were also recorded by the Fire Department of the City of New York between March 20 and April 5.
The figure was reported to be a nearly 400 percent increase from the same period last year, when the department received 453 calls for cardiac arrest patients who died.
The graphic below, provided by Statista, shows the number of confirmed COVID-19 cases, the disease caused by the new strain of coronavirus, in a selection of states.
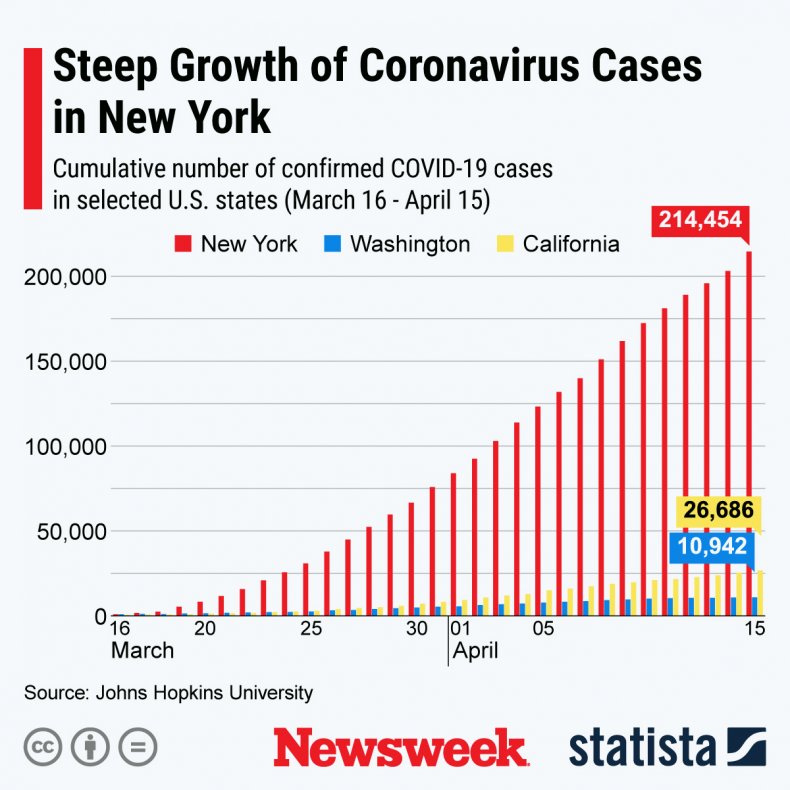
A chart provided by Statista shows the cumulative number of confirmed COVID-19 cases in New York, Washington and California from March 16 through April 15. STATISTA
Health officials in Massachusetts were said to have reported around 317 at-home deaths in March. The figure is reportedly a 20 percent increase from the same period over the past three years.
Officials in Detroit reported 150 "dead person observed" calls were received from April 1 to April 10. The number was said to be at nearly 40 during the same period for the past three years, according to city 911 call data.
It is hoped the quality of the figures will improve with further expansion of testing across the country. Hayward told Newsweek: "The CDC is responding to the need to accurately count COVID-19 deaths."
New Coronavirus Test Could Produce Results Six Times Faster Than CDC's
READ MORE
The CDC recently issued new guidelines for counting cases and deaths, which have been in effect from April 14.
"As of April 14, 2020, CDC case counts and death counts include both confirmed and probable cases and deaths," the CDC states on its website.
"State and local public health departments are now testing and publicly reporting their cases. In the event of a discrepancy between CDC cases and cases reported by state and local public health officials, data reported by states should be considered the most up to date," it adds.
Hayward noted: "The new guidelines in essence help identify probable COVID-19 deaths in the absence of testing – which is important."
The COVID-19 virus, which was first reported in Wuhan, China, has infected more than two million people across at least 185 countries and regions. Over 139,400 have died, while nearly 528,300 have recovered from infection, according to the latest figures from Johns Hopkins University.
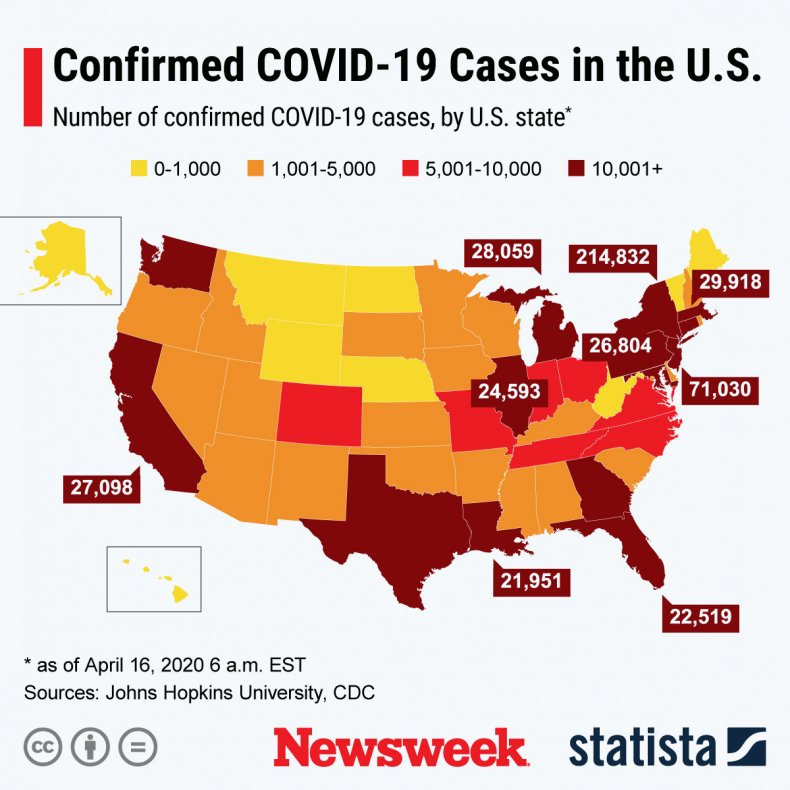
The graphic below, provided by Statista, illustrates the spread of COVID-19 across the U.S.
Health officials in Massachusetts were said to have reported around 317 at-home deaths in March. The figure is reportedly a 20 percent increase from the same period over the past three years.
Officials in Detroit reported 150 "dead person observed" calls were received from April 1 to April 10. The number was said to be at nearly 40 during the same period for the past three years, according to city 911 call data.
It is hoped the quality of the figures will improve with further expansion of testing across the country. Hayward told Newsweek: "The CDC is responding to the need to accurately count COVID-19 deaths."
New Coronavirus Test Could Produce Results Six Times Faster Than CDC's
READ MORE
The CDC recently issued new guidelines for counting cases and deaths, which have been in effect from April 14.
"As of April 14, 2020, CDC case counts and death counts include both confirmed and probable cases and deaths," the CDC states on its website.
"State and local public health departments are now testing and publicly reporting their cases. In the event of a discrepancy between CDC cases and cases reported by state and local public health officials, data reported by states should be considered the most up to date," it adds.
Hayward noted: "The new guidelines in essence help identify probable COVID-19 deaths in the absence of testing – which is important."
The COVID-19 virus, which was first reported in Wuhan, China, has infected more than two million people across at least 185 countries and regions. Over 139,400 have died, while nearly 528,300 have recovered from infection, according to the latest figures from Johns Hopkins University.
The graphic below, provided by Statista, illustrates the spread of COVID-19 across the U.S.
Failure to count COVID-19 nursing home deaths could dramatically skew US numbers
Thomas Perls
April 27, 2020 8.11am EDT
https://theconversation.com/failure-to-count-covid-19-nursing-home-deaths-could-dramatically-skew-us-numbers-137212
In New York state, 19 nursing homes have each reported 20 or more deaths from COVID-19. A nursing home in New Jersey reported 70 deaths out of its 500 residents. In the words of New York Gov. Andrew Cuomo, these homes have become a “feeding frenzy” for the virus and “the single biggest fear.”
With the clustering of people who are frail and have multiple other illnesses like heart disease, stroke, chronic lung disease and diabetes, the risk of severe illness and death from COVID-19 is much higher in nursing homes.
Yet, the United States does not know how many people are dying from COVID-19 in part because the government is only just now requiring nursing homes to start reporting numbers of presumed and confirmed cases and deaths to the federal Centers for Disease Control and Prevention.
The missing cases could dramatically skew the national death count. When France started reporting death data from some of its nursing homes, the daily COVID-19 fatality numbers almost doubled.
The Associated Press conducted its own survey in the U.S. and found there had been nearly 11,000 COVID-related nursing home deaths across the country as of April 24. However, just 23 states have been publicly reporting nursing home deaths. States also vary in how and where they are performing tests, and some count only proven cases and not also presumptive ones, leading to significant underestimates of the death toll.
As a geriatrician at Boston Medical Center and researcher at Boston University School of Medicine, I have watched in dismay as COVID-19 has become a deadly flash flood among the very old people I care for and study. I would not be surprised if the deaths in nursing homes at least double the U.S. COVID-19 death count.
In Massachusetts, 77% of nursing homes affected
Hints of what nursing homes and their residents and staff are going through have emerged from the states that have started publicly sharing data about them.
With Massachusetts Gov. Charlie Baker leading the charge, the Massachusetts Department of Public Health is providing a daily update on nursing homes where residents or staff have either tested positive or are presumed to be infected with COVID-19.
As of April 25, about 77% of Massachusetts nursing homes – 299 of 389 – had at least one case of COVID-19. That percentage will no doubt climb as the state carries out its mandated testing at nursing homes. About one-third of Massachusetts nursing homes reported more than 30 COVID-19 cases each among residents and staff.
Nursing homes are required to maintain infection prevention protocols to prevent the spread of infectious diseases into and within their facilities. But COVID-19, which is much more contagious than the flu, has punched holes in even the most careful and diligent facilities. Some nursing homes have also been in trouble for past problems with infection control.
It was initially estimated that on average, a person infected with COVID-19 led to an additional 2.5 people becoming infected. This basic reproductive number is called R0. A Los Alamos National Laboratory study released April 7 indicates that this earlier estimate is woefully low and that the R0 is more like 5.7. For comparison, the R0 for flu is around 2.
Among nursing home residents, the reproductive number is likely even higher than the average of 5.7. Many of the brave and caring staff in these nursing homes become infected, likely because of the intensity of this higher R0 and their exposure time with residents. By one report, nearly half of surveyed nursing homes reported staff staying home and not working because they had signs of or were proven to have COVID-19. The exposure to COVID-19 underscores how critical it is for nursing homes to get the adequate supplies of personal protective equipment they have been crying out for.
I believe it is likely that the majority of nursing homes throughout the U.S. and beyond have or will soon have multiple residents and staff who are COVID-19 positive. One large nursing home operator in Britain estimates that two-thirds of its homes have outbreaks.
We haven’t heard about most deaths yet
By the Centers for Disease Control and Prevention’s latest estimate, the U.S. has about 15,600 nursing homes with some 1.3 million residents. One quarter of those residents, about 425,000, are over the age of 80. In Massachusetts, the average age of death in confirmed COVID-19 cases is 82.
As of April 26, 56% of Massachusetts’ COVID-19 deaths occurred in nursing homes. The World Health Organization similarly estimates that half of COVID-19 deaths in Europe and the Baltics are among their 4.1 million nursing home residents. A minimum of 50% of the COVID-19 deaths occurring in nursing homes also agrees with the Kaiser Family Foundation’s review of data from the 23 states that are publicly reporting nursing home deaths.
The limited scope of counting people who have died from COVID-19 is not just a U.S. problem. A representative of British nursing homes, Care England, says that 7,500 people in nursing homes there have died due to COVID-19 – five times the U.K. government’s estimate of 1,600.
One indication of the high death toll from nursing homes comes from Belgium. The country has the highest per capita rate of COVID-19 deaths in the world – 57 per 100,000 people – primarily because officials there include nursing homes’ COVID-19 deaths in the national count and they are including both presumed and proven cases. Like Massachusetts, more than half of COVID-19 deaths in Belgium occur outside of hospitals.
The current U.S. rate, according to Johns Hopkins University, is 16 per 100,000, but its reports are only as reliable as its data sources, which include the CDC and state departments of health. This rate is likely lower than Belgium and 11 other countries because of the great variation across the U.S. in which data are not included, such as people who die outside of hospitals, and the data missing due to limited testing.
On April 19, the Centers for Medicare Services announced it would begin requiring U.S. nursing homes to report all confirmed or presumed COVID-19 cases to the CDC. I hope this will include past cases and deaths.
To get an accurate count, veterans’ homes, assisted living centers, group homes and other senior housing facilities must be required to report their past and current COVID-19 cases and deaths, as well.
There is plenty we still do not know about for why nursing home residents have borne the brunt of this pandemic. As Gov. Baker has indicated, “This is a topic that will get a lot of appropriate analysis after the fact.”
CONGRESS QUIETLY BOOSTS SPENDING ON LAWMAKERS’ EXCLUSIVE CONCIERGE HEALTH CLINIC
Lee Fang
https://theintercept.com/2020/04/29/coronavirus-congress-health-clinic/
IN MID-MARCH, Rep. Mario Diaz-Balart, R-Fla., became one of the first lawmakers to announce he had Covid-19, after testing positive for the disease caused by the novel coronavirus.
He received his diagnosis promptly from congressional doctors employed by the Office of the Attending Physician, and recovered by early April. Coronavirus testing was made available early and often for members of Congress, who enjoy concierge medical services courtesy of a world-class government health clinic.
Diaz-Balart, like many other voices on Capitol Hill, has denounced increased public spending on health services as a dangerous “government takeover of healthcare.” But like every lawmaker, he enjoys gold-plated medical care from OAP, which provides on-call services at taxpayer expense — and recently got a boost in funding.
Just months before the pandemic, lawmakers hiked funding for the OAP clinic, a move that has not been previously reported. The last congressional appropriations bill, passed in December, increased the budget for the office to $3,868,000 this year. Then, in March, the CARES Act, the sweeping $2.2 trillion bailout legislation, included a special provision that appropriated an additional $400,000 to the OAP clinic as part of a package of special funds to prepare the capital for coronavirus response and hygiene.
All together, the OAP budget has increased more than 25 percent over the last decade. The move to secure the health and safety of lawmakers contrasts sharply with the policy focus of Congress, which has largely faced a stalemate over the expansion of low-cost health care services over the last decade. In the first weeks of the pandemic, few had access to the same rapid Covid-19 testing that was made available to lawmakers through the clinic.
THE OAP has been described as “some of the country’s best and most efficient government-run health care.”
Lawmakers are only charged around $600 in annual fees, which covers a small fraction of the costs for OAP operations. The vast majority of the budget comes from money delegated by the federal government. Even the low flat rate isn’t necessarily required. Some lawmakers who have declined to pay the nominal fee are not turned away from the clinic, according to previous reports.
The clinic, managed by Dr. Brian Monahan, a rear admiral in the Navy, employs three doctors, a pharmacist, and over a dozen nurses and medical technicians. The clinic not only provides coronavirus testing, but routine flu vaccines, lab work, physicals, and a range of emergency treatments. Lawmakers have claimed that they use the OAP office as their primary care physician. It also also treats some medical emergencies among tourists.
Members of Congress also receive regular physical therapy care at the clinic. An on-site radiology suite provides X-rays. Specialty doctors from military hospitals routinely visit the OAP at no extra charge, while lawmakers are often referred for free outpatient care at the Walter Reed National Military Medical Center.
In recent weeks, the OAP has played a critical role in helping lawmakers respond to the rapid spread of coronavirus. Sen. Rand Paul, R-Ky., and other lawmakers who tested positive have consulted closely with doctors from the OAP on ways in which to quarantine themselves and recover.
The office has taken the lead on producing public health policies for congressional operations during the coronavirus pandemic. A recent congressional guidance issued by OAP advises the proper use of face masks in the capital and the use of the gallery space above the House of Representatives to facilitate social distancing.
The CARES Act also provided $12 million for the Capitol Police and an additional $25 million for capital construction crews to prepare sanitation supplies for the administration of congressional buildings.
Dale Fountain, the chair of Enact Universal Healthcare for California, a single payer advocacy group, said he was disappointed to learn about Congress moving to shore up its own taxpayer-funded health care.
“Speaker Pelosi has been adamant in her rejection of single payer for everyone,” said Fountain, noting that the omnibus spending bill in December repealed three tax provisions of the Affordable Care Act while boosting the OAP.
“It has been obvious for awhile that when it comes to her own healthcare and her own projects, ‘how will we pay for it?’ was never a concern,” he added.
Boris Johnson’s Coronavirus Lies Are Killing Britons
Sonia Faleiro
https://theintercept.com/2020/04/30/boris-johnsons-coronavirus-lies/
“THE NHS SAVED my life, no question,” Boris Johnson said earlier this month, publicly thanking Britain’s beloved National Health Service for successfully treating him for Covid-19 over a seven-day period in early April. “It’s hard to find words to express my debt,” the prime minister said, naming several nurses, and thanking two in particular for standing by his bedside for 48 hours when “things could’ve gone either way.”
Johnson’s speech, which he might have hoped would be lauded for its graciousness, served instead as a reminder that the NHS is a success despite him. When the first cases of Covid-19 in the U.K. were confirmed in late January, Johnson’s Conservative Party government claimed that it was prepared for any eventuality.
That turns out to have been a lie. The government’s failure to provide sufficient protective gear, which has so far contributed to the deaths of at least 114 health care workers in Britain, was preventable. Moreover, two separate investigations have now revealed high-level attempts to cover it up.
Earlier this week, the BBC’s Panorama showed that the British government’s pandemic stockpile lacked key equipment, such as gowns, visors, swabs, and body bags. The government was of course aware of this deficit and yet, even after the pandemic hit the country’s shores, U.K. leaders refused multiple opportunities to bulk-buy PPE. When the lack of supplies became obvious to the public, the government tried to hide the problem by inflating PPE numbers, counting one pair of gloves as two items of PPE.
Another investigation, by the Sunday Times, a decidedly right-leaning newspaper owned by Rupert Murdoch that has previously swooned over Johnson, calling him a “rockstar,” showed just how casually the prime minister confronted the pandemic. Johnson had skipped five high-level emergency meetings to discuss the virus, the newspaper reported. He insisted, in a manner reminiscent of U.S. President Donald Trump, that briefing reports be as short as possible. He went on holiday to a country estate, refused to work weekends, and attended a fundraising ball.
After his thank-you speech, Johnson retired to Chequers, the lavish 16th century, 1,500-acre manor house used by British prime ministers, where he was photographed strolling the grounds with his pregnant fiancée and their Jack Russell terrier. (The couple’s baby boy was born on Wednesday.) The world was in the grip of an unprecedented crisis, but the U.K. was without a leader.
Johnson’s NHS caregivers, meanwhile, returned to work immediately, and every day, reports stream in of front-line health workers like them who are forced to combat the highly contagious virus in clinical waste bags and plastic aprons. They are asking schools to donate science goggles. They are adapting snorkels as respirator masks. When UNISON, the U.K.’s largest public services union, opened a PPE alert hotline, it was flooded with calls from health care workers who talked about having to buy their own equipment.
Of the health care providers who have died so far, one, Abdul Mabud Chowdhury, a consultant urologist in London, had written a Facebook post appealing to Johnson to protect him and his co-workers. “I hope we are by default entitled to get this minimal support,” he wrote on March 18, five days before he was hospitalized.
Johnson is responsible for his death, and for the death of every other health care worker in the country.
THE FIRST SIGNS that Johnson was out of his depth emerged early on in the pandemic. While repeating that the government was “led by science,” the newly elected prime minister seemed to be pushing a dubious “herd immunity” strategy, hoping that exposure would build immunity among the British public, an outcome that, happily for Johnson, would require no action from his government. The meetings of the prime minister’s scientific advisory board, which strives to impartially inform the government’s response based on science, were attended by his chief adviser. The adviser is said to have actively participated, thereby undermining the neutrality of the process, and raising public concerns that decisions were made to suit political objectives rather than scientific ones.
While Johnson talked about science, his actions were those of a man convinced that he, and by extension, the country he led, possessed the magical ability to escape a disease that had brought much of the world, including neighbors like France, Spain, and Italy, to its knees.
In February, the European Centre for Disease Prevention and Control had warned that for the most serious cases of Covid-19, health workers would need around 20 sets of PPE per patient per day. The Johnson government was given as many as three opportunities to participate in an EU scheme to bulk-buy PPE. It chose not to. In fact, British officials shipped more than 200,000 units of PPE to China, then lied about choosing not to participate in the EU scheme, claiming they had “missed the emails” despite having attended meetings about the acquisition. In a TV interview, Johnson spoke of how one strategy for confronting the novel coronavirus could be to “take it on the chin.”
In early March, Johnson and his fiancée attended a rugby match. Later, he met with hospital patients, some of whom, he said, may have had Covid-19. He bragged about shaking their hands.
In March, South Korea, Taiwan, and even small Indian states like Kerala had showed how democratic societies, working doggedly, could use a dedicated World Health Organization-approved program of contact tracing, testing, and isolation to contain the virus. Some experts said that given how long it might take to develop a vaccine — as long as five years, perhaps — such a program was the only realistic way forward. New Zealand’s Jacinda Arden and Germany’s Angela Merkel also employed these tools early on; by acting quickly, they saved lives.
These countries’ successful actions were presented to Johnson on a platter. The U.K. had a head start over many others — as much as nine weeks, according to one expert, or the time between human to human virus transmission being confirmed in China and the U.K.’s first known case of local transmission on February 29. But busy with Britain’s departure from the EU on January 31, Johnson ignored every warning and squandered every opportunity to protect his country. Born and bred into the idea that he was exceptional, he endangered himself along with millions of Britons, many of whom imbibed his magical thinking.
On March 16, organizers of the four-day Cheltenham Festival, a horse racing event, cited Johnson’s presence at the rugby match earlier that month as the reason to go ahead with their event, noting that “the government guidance is for the business of the country to continue as usual.” The races attracted some 250,000 people over four days, many of whom have since tested positive for the virus. The hospitals in Gloucestershire, the county where Cheltenham is located, are now among the hardest-hit in the country.
The government also left borders open, allowing flights from Italy, China, and the U.S. without any quarantine restrictions until late this month, long after most other countries had begun to quarantine arrivals. On Johnson’s watch, the U.K. is a staggering example of what not to do.
The rising death toll in Britain, for which Johnson is personally responsible, makes it impossible to believe anything he says moving forward. To believe him could mean endangering your own life and the lives of your loved ones. In the absence of trustworthy leadership, people are being forced to make critical decisions alone. This daily struggle is taking place in the midst of another calamity — an economy that was already severely damaged as a result of Brexit is now crumbling due to the pandemic.
The UK economy will shrink by 6.8 per cent as a result of the coronavirus outbreak, and it will take three years to recover. Despite this, the U.K.’s chief Brexit negotiator has made it clear that he will not seek an extension on the December 31 deadline to reach a trade agreement with the EU. If no agreement is reached, the country will be forced to revert to World Trade Organization terms, making it liable for tariffs and border controls that will further strain the economy.
This is something Britain can ill afford. Just three weeks after the nationwide lockdown began on March 23, more than 1.5 million Britons were facing food insecurity, according to a study; this figure includes 53 percent of NHS workers. The study also said that 830,000 children could be going without the free school meals on which they relied because the government had failed to keep yet another promise — to feed children in need during the lockdown.
THE CURRENT CRISIS has been a decade in the making. Johnson and his Tory colleagues have spent years undermining the NHS, using the excuse of austerity measures to cut salaries and reduce benefits, when in reality they appear to have been trying to push the country toward a U.S.-style private health care system.
In 2011, five Tory members of parliament, three of whom are now ministers in Johnson’s government, published a pamphlet advocating for privatization. According to a Guardian investigation, private firms were given contracts worth £15 billion, about $18 billion, a jump of 89 percent since 2015. In the years that followed, Johnson’s predecessor, Theresa May, scrapped nursing grants, which help nurses with study and living costs, and rejected salary increases, voting to keep nurses’ salaries below the rate of inflation. Johnson, and virtually every other member of the Conservative Party, voted with May and cheered after the votes were announced. May explained the decision to a nurse’s face, saying in her typically bloodless way: “There isn’t a magic money tree we can shake.”
In 2016, the Tory-led Brexit referendum poisoned the atmosphere for EU citizens in the U.K. so much that more than 11,000 immigrant NHS workers, including 4,763 nurses, went back home. “It’s the National Health Service, not the International Health Service,” Matt Hancock, Johnson’s health minister, sneered on Twitter at the time. The outcome of Hancock’s shortsightedness was revealed last month, when he was reduced to begging retired health workers, including those in their 70s and 80s who are most vulnerable to the virus, to return to work to boost staff numbers. (Hancock contracted the coronavirus in March.) One of the emergency hospitals he helped set up to deal with Covid-19 has remained largely empty for lack of nursing staff.
Johnson, for his part, went out of his way to praise the two immigrant nurses who cared for him while he was ill, one from New Zealand and the other from Portugal. A new scheme aimed at boosting staff numbers during the crisis allows foreign doctors, some of whom are living as refugees in the U.K., to join the NHS, but only as support staff, not as doctors, even though they are fully qualified back home.
And all this time, the Tories were steadily undercutting the national medical stockpile, reducing its value by almost 40 percent in three years while also privatizing its management. The last rehearsal for a pandemic, in 2016, had predicted the health service would collapse, according to the Sunday Times investigation. In the years that followed, the newspaper reported, “preparations for a no-deal Brexit sucked all the blood out of pandemic planning.”
THE DEATH TOLL in the U.K. stands at 26,771 as of April 30, according to the government. (The official figures now take into account deaths in private homes and nursing homes rather than only in hospitals.) A Financial Times analysis of data from the Office of National Statistics showed that earlier figures didn’t account for these additional numbers and that as of last week, according to the paper, the true number of deaths was closer to 41,000.
It is tempting to believe that Johnson’s brush with the virus has taught him humility or that the investigations have shamed him into doing his job. But some NHS workers weren’t impressed by his expressions of gratitude.
“This outpouring of emotion helps the government gloss over the shortages,” one health worker told the BBC. “Calling us heroes just makes it OK when we die.”
On Monday, after three weeks away, Johnson returned to work. At a press conference outside 10 Downing Street, he was in a self-congratulatory mood, speaking of “real signs now that we are passing through the peak.” The numbers suggest otherwise, and there was only a passing mention of PPE.
As the U.K.’s death toll threatens to be the worst in Europe, there really is just one choice. Boris Johnson must apologize, resign, and let a real leader take charge.
SMALL FARMS, ALREADY STRESSED AND UNDERFUNDED, STRUGGLE FOR FEDERAL CORONAVIRUS RELIEF
Rachel M. Cohen
https://theintercept.com/2020/04/29/small-farms-coronavirus-aid/
BEFORE CORONAVIRUS HIT, farmers in the U.S. were already hurting from years of falling food prices, severe weather, and, more recently, President Donald Trump’s trade war. “We’ve had a record number of farm bankruptcies [in the U.S.], total farm debt is at $425 billion, [and farmer] incomes have fallen by about half since 2013,” said Eric Deeble, policy director at the National Sustainable Agriculture Coalition, which supports small and mid-sized family farms.
Now, with the global pandemic closing factories and restaurants and disrupting supply chains, already stressed farms are grappling with lower demand and fewer markets to sell in, as well as a presidential administration that favors relief for big businesses over small. Small farmers in particular — those who sell directly to farmers markets, schools, and other local food hubs — are facing an existential crisis, as they face slim odds of accessing competitive federal stimulus money.
They have reason to be pessimistic. In recent years, federal subsidies to help struggling farmers have flowed almost exclusively to large corporate farms. Of the roughly $28 billion the Trump administration has distributed to food producers to offset losses from his trade wars, almost all went to big farms.
Advocates for small farmers say this is driven in part by the preference of Trump’s agriculture secretary, Sonny Purdue, who has encouraged farmers to get bigger farms if they wanted to stay in business. “Big get bigger and small go out … and that’s what we’ve seen,” he told a group of Wisconsin dairy farmers in 2018, echoing Richard Nixon’s agriculture secretary, who infamously told farmers in the 1970s to “get big or get out.” While 91 percent of U.S. farms are small — defined by the federal government as an operation with gross cash income under $250,000 — large farms account for 85 percent of the country’s farm production.
The public health crisis has already had a devastating impact on agriculture across the country. A report released in mid-March by the National Sustainable Agriculture Coalition estimated that small farms would see a $689 million decline in sales from March to May this year due to Covid-19, leading to a payroll decline of $103 million and a total loss to the economy of $1.3 billion. Now, as the pandemic shows no sign of slowing, the coalition worries that the impact for small farmers will be even more substantial — which could lead many small farms to permanently close.
Under pressure from groups like the National Sustainable Agriculture Coalition and the National Farmers Union, Congress did work to address some of the needs of small and direct-market farmers in the $2 trillion Coronavirus Aid, Relief, and Economic Security, or CARES, Act, signed into law on March 27. While lawmakers did not include all that advocates pressed for — like emergency food purchases from small processors and direct payments to small farms — the CARES Act did allocate $9.5 billion to farmers and said some (unspecified portion) of that amount should go to “producers that supply local food systems, including farmers markets, restaurants, and schools.”
But in the weeks following the CARES Act, farmers struggled to access any relief, as the agriculture aid stalled and many farmers found themselves ineligible for the Small Business Administration emergency loans. On April 10, 33 senators sent a bipartisan letter to Purdue, urging the USDA to follow the CARES Act and distribute federal aid to small farmers specifically. A week later, when the USDA finally announced how it planned to allocate the $9.5 billion from the CARES Act, it appeared that no money would be reserved specifically for small farmers.
In a statement provided to The Intercept, a USDA spokesperson said the department planned to provide assistance to “most farms” that experienced at least a 5 percent loss. To ensure that funding will help small farms, the USDA said it “is utilizing payment limits and [adjusted gross income] eligibility criteria that were used by Congress when developing the 2018 Farm Bill” — the same bill that left small farmers in the lurch over the last two years. The spokesperson also said that the USDA planned to use a $900,000 AGI limit for those who do not make 75 percent or more of their income from farming — a notably high threshold considering that small farmers earn between $1,000 and $250,000 from their farms.
“Bailout money always goes to the big farmers, the people who produce soy and crops and sell into commodity markets,” said John Peck, executive director of Family Farm Defenders, a national organization that supports sustainable agriculture. “This is all part of our country’s cheap food policy where we basically subsidize capital-intensive, large-scale industrial farming.”
Farmers who sell directly to consumers or participate in regional food hubs typically don’t rely on federal subsidies.
“Small diversified farmers are pretty effective at doing what they do, which is finding markets and filling them, and haven’t required a lot of support,” said Deeble. “But the flip side is if you’re usually good in normal times and don’t rely much on the government, it can be harder to get government help when you need it.”
J.D. Scholten, a Democratic House candidate running in Iowa’s 4th Congressional District, said there’s still a lot of uncertainty about how the federal stimulus money will be allocated, “but what we’ve seen [since the trade wars] is that Secretary Purdue gets to dictate who gets bailed out and who doesn’t, and there’s not a lot of oversight.”
Colby Ferguson, a small farmer and the director of government and public relations for the Maryland Farm Bureau, defended the bulk of federal subsidies flowing to large farms. “They should get most of the money since they generate the most volume of our food supply,” he said. “If we didn’t help the big guys, that would also affect the small guys.”
The Farmers Market Coalition, a nonprofit that supports local markets across the country, has also been pushing for emergency aid and a federal declaration that farmers markets should be allowed to operate as essential businesses. (California has deemed farmers markets essential, but other states have shut them down or left it more ambiguous.) Advocates say open-air markets can serve as a safer way to buy groceries during the pandemic.
“If farmers markets go out of business that means local farmers lose access to those consumers,” said Ben Feldman, executive director for the Farmers Market Coalition. While American food purchasing has swiftly shifted during the pandemic from restaurants to grocery stores, it is typically much harder for small farmers to sell their products to large grocery stores.
“I don’t want to be alarmist, because farmers market operators, like the farmers who sell to them, are very resilient and adaptable and do an incredible amount with very limited resources,” said Feldman. “But this could definitely force markets to close.”
According to the USDA, local food sales more than doubled between 2012 and 2017. But profit margins for small farmers remain low or nonexistent, and most small farmers also have other jobs.
Peck of Family Farm Defenders said he worries this pandemic will be exploited by big corporations to crush the local food movement and correspondingly wreak further damage on the climate. “To feed the world and cool the planet, we need to move away from industrial agribusiness,” he said.
Some advocates say they’re cautiously optimistic that the next stimulus bill could offer more help to small farmers and noted that there’s been growing public awareness of the risks posed by our global supply chain and the need to invest in a more resilient food system.
Scholten, who has been sounding the alarm for years about the risks of monopolized agriculture, said the pandemic exposes how “dangerously dependent” we are on imports. “We’ve had these ‘get big or get off the farm’ policies for years,” he said. “But I think there’s huge potential now to regionalize our food production, localize it.”
“In the 4th District of Iowa, the second-most agricultural producing district in the nation, we have only two farm-to-table restaurants; we have small towns losing their grocery stores because Dollar General is coming in and undercutting them, but they don’t sell fresh produce and meats, and we have farmers not making a dime,” he said. “So who are we doing this [production] all for?”
The Corporate Right Is Giving Us Two Choices: Go Back to Work, or Starve
Jon Schwarz
https://theintercept.com/2020/04/29/coronavirus-government-right-bailout/?utm_medium=email&utm_source=The%20Intercept%20Newsletter
The GOP and its core constituents — conservative corporations — now face two dangers, one in the short term and one in the longer term. They’re currently using their standard playbook to smother both. Whether they succeed will determine our lives for decades.
The short-term danger is that Americans will resist the push from business to get us back on the job and making money for them. Their plan is simple: Starve us out. They know we can’t survive indefinitely without a continuing government bailout focused on regular people’s needs. So they’re going to stop that bailout from happening.
The longer-term danger they face is that we’ll make the government work for us in the short term — and then we will realize we could make it work for us all the time by removing the threat of starvation from their arsenal. This would totally change the balance of power in society. This is their deepest fear, one that’s consumed them since World War II, the first time in history that everyday people gained consciousness that it was possible for them to use the government to create a world that puts them first, not their bosses.
In the short term, they will just say that America is now, sadly, out of money. At a recent press conference, Senate Majority Leader Mitch McConnell, R-Ky., still metaphorically drenched from the firehose of cash he sprayed all over Wall Street and big American business during the past month, looked mournful. Money for state and local governments so they’re not forced to lay off massive numbers of teacher and firefighters? Hazard pay for doctors and nurses? Help for people paying rent? Sorry, no. “Until we can begin to open up the economy,” McConnell said, “we can’t spend enough money to solve the problem.” The same thinking prevails in the Trump administration, particularly about money for state and local governments.
The strategy is already bearing fruit, with states such as Florida, Georgia, Texas and Tennessee easing restrictions on business — all to the approval of various presidential tweets.
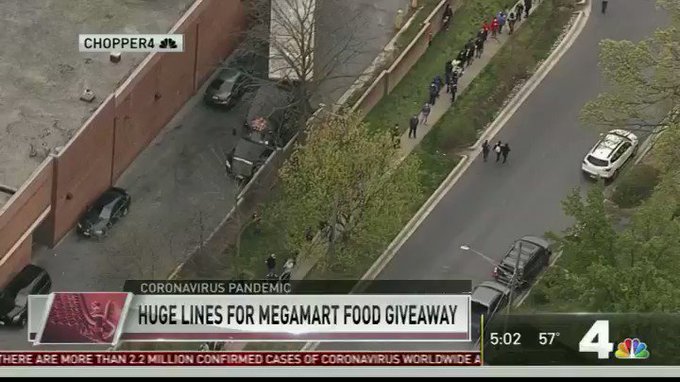
To understand the depths of this depravity, watch this local news helicopter footage of hundreds of people in Rockville, Maryland — just outside of Washington, D.C. — close together in line for free food being given out by a Megamart Supermarket. The station’s correspondent said that “in this whole plan, of what we do for people during this pandemic … these are perhaps people who are not seen.”
But this is wrong. America’s corporate right absolutely sees these people. Like any competent group of thieves robbing a bank, they see the vulnerable as hostages.

Joyce Karam
✔@Joyce_Karam
Chilling footage from Maryland, US where hundreds are lined up to get a free bag of food or $30 voucher from store.
Lines wrapping around parking lot and building itself, show extent of desperation:
17.8K
5:10 PM - Apr 17, 2020
Twitter Ads info and privacy
12.7K people are talking about this
Anyone who knows the Washington, D.C., area would find the supermarket scene nauseating, shocking, and completely predictable, all at the same time.
Rockville is in Maryland’s Montgomery County, one of the richest counties in the United States, with a median income of about $100,000. Georgetown Prep, the private school attended by Supreme Court Justice Brett Kavanaugh — current day student tuition $38,330 — is a modest stroll from this particular Megamart. The headquarters of Lockheed Martin — which paid its CEO $21.5 million in 2018 and gets 70 percent of its revenue from the federal government — is a 10-minute drive away. Then if you need a new ride, you’re not far from Bethesda Euromotors, where you can pick up a Mercedes SUV for $170,000.
The people who actually make the lives of Montgomery County’s aristocrats run are generally invisible to the aristocrats themselves. But here, many were suddenly in one place: visible and desperate. The county’s princelings and princesses are a big chunk of the elites who truly control the United States. They unquestionably have the power to end the desperation. They just won’t.
Why? It’s easy to conclude they simply don’t care whether workers live or die; certainly President Trump’s demand that meat processing plants stay open even as the people inside them get sick makes that as clear as anything could. But it’s more complex than that, and in fact more dreadful.
There are two paths forward during this pandemic. The U.S. could rationally follow the science about the novel coronavirus, as complicated and incomplete as it is. This would necessitate putting much of the economy in hibernation until we have the capacity to immediately find anyone with Covid-19 and provide them with a safe place to stay in quarantine, while doing our best to keep everyone who has to work safe. For regular people to survive, we would need government action along the lines of that proposed by Sen. Bernie Sanders, I-Vt., and Rep. Pramila Jayapal, D-Wash.: guaranteeing no one goes hungry, direct emergency cash payments to everyone, Medicare covering all health costs.
Alternately, we can follow the heart’s desire of the corporate right, and shove everyone back to work as soon as possible.
The problem for the corporate right is that the force-everyone-to-risk-death concept is unpopular. Recent polls show overwhelming support for the continuation of shelter-in-place policies until public health officials say it’s safe to lift them.
This could easily change, however, as the Rockville scenes make clear. A $1,200 stimulus check will pay for less than one month of the median U.S. rent for a two-bedroom apartment. GOP governors are already maneuvering to make it difficult for constituents scared that their job might kill them to access the expanded unemployment benefits of the CARES Act.
What we can expect to see on the right is ever-more ostentatious wailing and rending of garments about the suffering of the jobless. Jeanine Pirro has already explained on Fox that “for every percentage of increase in unemployment, there is an increase in deaths from suicide, alcoholism, domestic violence, and a loss, and depression.” USA Today columnist Glenn Harlan Reynolds wrote about the “class divide here … between the people in the political/managerial class on the one hand and the people in the working class on the other.”
This weepy concern for the unemployed will be bogus, but the suffering will be absolutely real, because the right will make sure it is.
The corporate right’s hoped-for dynamic recently was explained explicitly by Trevor Burrus of the Cato Institute, a conservative D.C. think tank: “The economic and human devastation is difficult to contemplate, and it’s only getting worse. … Many will hit a point where the trade-off will be between possibly getting COVID-19 and being able to feed their families. The disease doesn’t look so bad then.”
There it is: The choice being given to regular Americans will be to work or die.
In Adam Smith’s “The Wealth of Nations,” probably the most famous book ever written about economics, Smith explains that the “masters of mankind” (rich employers and financiers) always have known this is the choice available for most people. When workers fight back against the masters for more pay or better conditions, their efforts “generally end in nothing, but the punishment or ruin of the ringleaders.” Much of this is due to “the necessity which the greater part of the workmen are under of submitting for the sake of present subsistence.” That is, working people just can’t withdraw their labor for long, or they’ll go hungry.
The problem, from the corporate right’s perspective, is not just that business would lose its cudgel for the moment if the U.S. government pays people to stay home. (To understand why we can afford it at unusual times like this, read about Modern Monetary Theory, which is often condemned as a radical heresy but is in fact just a straightforward description of reality.) The deeper long-term peril, from the perspective of Wall Street and big business, is that normal Americans will realize they can use the government to eliminate the “necessity” of which Smith wrote — and thereby permanently alter who holds power in U.S. society.
This was famously explained in a 1943 essay by Michal Kalecki, a Polish economist, titled “Political Aspects of Full Employment.” At that moment, World War II was demonstrating for everyone with eyes to see that governments could end depressions and create economic booms via the straightforward method of spending money on basic human needs. There was no technical reason this couldn’t continue after the war, Kalecki wrote. But there was a huge political problem: An economy in which people could live without fear of unemployment would mean employers would no longer hold the whip hand.
As Kalecki put it, in a standard capitalist economy, the level of employment depends on the “confidence” of employers, and hence they must be catered to constantly. However, “once the government learns the trick of increasing employment by its own purchases, this powerful controlling device loses its effectiveness. Hence budget deficits necessary to carry out government intervention must be regarded as perilous.”
Kalecki’s key insight was that big business cares more about power than money. “It is true that profits would be higher under a regime of full employment than they are on average under laissez-faire,” he said, “but ‘discipline in the factories’ and ‘political stability’ are more appreciated than profits by business leaders. Their class instinct tells them that lasting full employment is unsound from their point of view.”
This perspective — that governmental power was enormous and could be used for the many rather than the few — was obvious at the time in 1940s. But it was forgotten over the next few decades, because powerful people wanted it forgotten. At various points, it’s been rediscovered, as by the civil rights movement during the 1970s. What we need now is slightly different than what Kalecki described: “full employment” with many people essentially “working” at not getting sick or infecting others. But the principle is the same, as is the terror that this possibility elicits on the right. They will do everything possible to make sure we forgot they just suspended all of their purported rules for as long as it took for them to unlock the U.S. Treasury and help themselves to trillions of dollars.
Now, with that accomplished, Republicans and the corporate right will pretend it never happened, suddenly reimpose the “rules,” and fight to the death against any genuine bailout for regular people. This will be the case even if such a bailout would probably be more profitable for business than a shambolic, disastrous reopening of the economy. From the point of view of the masters of humankind, it’s worth any number of dead Americans to stop us from asking: If we can use the power of the government on a huge scale in a crisis like this, what else can we do?
Subscribe to:
Comments (Atom)